What Was Done?
Global Problem Addressed
Appendicitis is the most common cause of urgent abdominal surgery among children. In the U.S., approximately 53,000 children undergo appendectomy each year for acute appendicitis.1, 2 Despite a substantial amount of research and vigorous debate, there is no consensus regarding the optimal postoperative management of these children. Therefore, wide variation exists amongst pediatric surgeons and presents an opportunity for quality improvement endeavors.3,4
Identification of Local Problem
Appendectomy is a targeted procedure for the ACS NSQIP Pediatric Project, so institution-specific and national statistics are readily available. Following the first year of participation, it was recognized that UC Davis was amongst the highest quartile for length of stay (LOS) despite a lower postoperative complication rate than other institutions. Our patients had an average length of stay of 3.6 days compared with 2.6 days nationally. This was more pronounced for patients with complicated appendicitis who had an average length of stay of 6.5 days compared with 4.7 days nationally. Since postoperative complications could not account for the prolonged average length of hospitalizations, the most likely contributors were variability in postoperative management and inconsistent criteria for discharge.
How Was the Quality Improvement (QI) Activity Put in Place?
Context of the QI Activity
The UC Davis Medical Center is a tertiary referral center with a large catchment area that includes parts of Northern California, Southern Oregon, Nevada, and Idaho. It also serves as the primary teaching hospital for the UC Davis Medical School, with a wide range of residencies and fellowship programs. The adjoining UC Davis Children's Hospital offers comprehensive pediatric care, is the region's only Level 1 pediatric trauma center, and is the only Level 1 children's surgery center on the west coast, as verified by the American College of Surgeons. Over the year prior to the implementation of this initiative, 128 children underwent appendectomy for acute appendicitis, of which 58 (42%) were found to have complicated appendicitis.
The UC Davis Office of Graduate Medical Education encourages quality improvement endeavors, particularly multidisciplinary and interdepartmental projects, and offers grant funding through a competitive application process. Grant recipients are provided both financial and technical support to assist implementation. Intermittent updates are required to ensure progress is being made.
Planning and Development Process
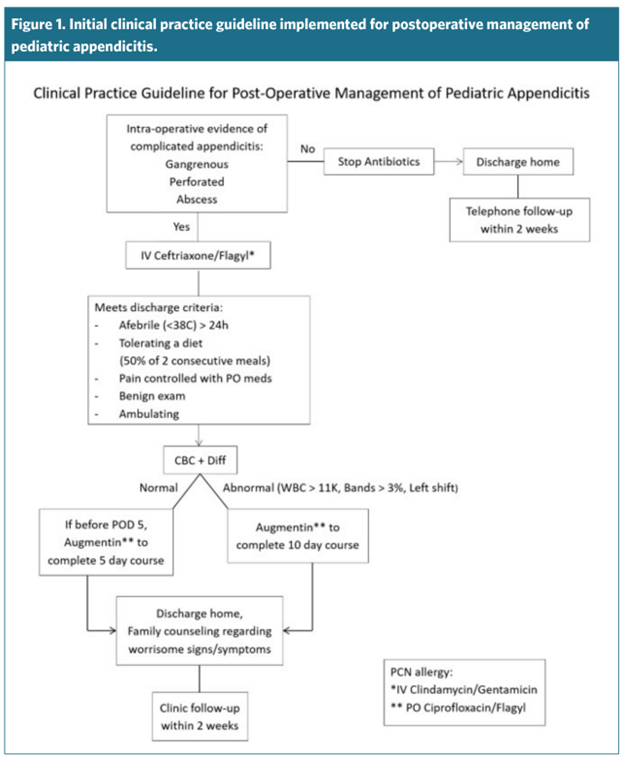
Clinical practice guidelines have been described at other institutions and their use, in general, has been endorsed by the American Pediatric Surgical Association.5 Guidelines used at several other institutions were obtained and a literature review performed to guide development of a unique, local clinical practice guideline. The directors of Pediatric Antimicrobial Stewardship provided recommendations for postoperative antibiotic regimen, taking into consideration the local antibiogram. A first draft of the local clinical practice guideline was presented along with local performance metrics to the pediatric surgery department during a weekly departmental meeting. Individual meetings were then held with each pediatric surgeon to elicit detailed concerns and discuss potential alternatives to specific elements. The guideline was revised based on the accumulated feedback and subsequently received unanimous approval. The final approved guideline defined complicated appendicitis by specific intraoperative findings, established clear discharge criteria, and specified the postoperative antibiotic regimen.
Description of the Quality Improvement Activity
Once the clinical practice guideline was approved, it was disseminated by e-mail to all members of the pediatric surgery team, including surgeons, residents, nurse practitioners, and pharmacists. Laminated badge buddy cards were also distributed, and the guideline was posted in each of the resident work rooms and call rooms. An e-mail explaining the project and its background, along with the current iteration of the guideline, was sent to rotating residents a few days prior to the start of each rotation. Surgeons, rotating residents, and nurse practitioners were primarily responsible for ensuring that the guideline was followed.