How Was the Quality Improvement (QI) Activity Put in Place?
Context of the QI Activity
Richmond University Medical Center is a Level 1 adult and Level 2 pediatric ACS TQIP-verified trauma center with 448 licensed beds providing care to an urban/ suburban community in Staten Island, NY. The trauma service alone cares for approximately 1,500 adult and 200 pediatric patients per year. Last year, out of 1,751 adults and children evaluated by trauma, 1,194 were admitted.
For this project, there was no hospital-wide oversight. The motivation behind this project was to improve upon our patient management, which would be reflected in our TQIP scores. But by initiating this conversation, we were able to bring more attention and awareness to the situation at hand. Seeing the success of our nurse-driven policy, the hospital system adopted our practice to assist in the reduction of CAUTls throughout the institution. Further motivation has encouraged other departments and programs to work collaboratively with trauma and constructively think of other measures to put in place for further improvement of patient management.
Planning and Development Process
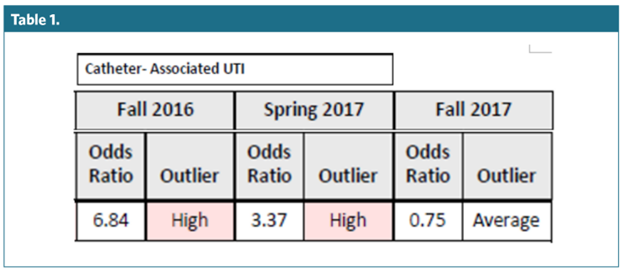
Based on the 2016 TQIP report, CAUTI was identified as an area of improvement. Once we settled on CAUTls, we constructed the nurse-driven Foley catheter protocol. The first unit educated on the new policy was the surgical intensive care unit (SICU). The nurses and nurse management staff on this unit were very open to the education and implementation. A discussion regarding all expected outcomes was had at the trauma committee meeting so that all stakeholders throughout the institution were on the same page. Once the staff was educated, we began daily rounding on all trauma patients in all units to see who fit the criteria for removal. After seeing the drastic reduction in CAUTls from the fall 2016 to spring 2017 report, more units bought in to the project, and we were able to train them as well. Currently, all units that intake trauma patients are trained on this policy.
The Nurse-Driven Foley Removal diagram was created by our trauma medical director and agreed upon among physicians within the hospital (Figure 1). This diagram is one of the crucial elements in this policy.
Description of the Quality Improvement Activity
Based on the benchmark findings in the TQIP report, it was evident that a performance improvement measure was needed. A Foley catheter management protocol was constructed to highlight the interventions implemented to manage this complication. Included in the policy is a CAUTI Reduction Bundle, Nurse Driven Foley Removal protocol, and daily rounding as a method to document and identify patients who no longer need Foleys. In addition, Foleys placed in the emergency department must be changed or exchanged within 24 hours of placement for traumatically injured patients. Also included in the protocol, the trauma and surgical team will utilized a Texas catheter in patients who fit the criteria. Daily morning rounds would be conducted on all trauma patients admitted to evaluate the care plan and see how to improve overall management and care. The education was provided by the trauma director and trauma team.
This policy was implemented on August 1, 2017.