How Was the Quality Improvement (QI) Activity Put in Place?
Context of the QI Activity
Henry Ford Allegiance Health (HFAH) is a 475-bed health system in Jackson, Ml. It is one of six hospitals in the Henry Ford Health System (HFHS) headquartered in Detroit, Ml. It is comprised of more than 40 different facilities and reaches residents in the counties of Jackson, Hillsdale, Branch, Lenawee, Ingham, Calhoun, Washtenaw, and beyond. Henry Ford Allegiance Health is committed to long-term lung health in our community. We are proud to be designated as a Lung Screening Center of Excellence by the Lung Cancer Alliance. With this designation, the Lung Cancer Alliance recognizes Henry Ford Allegiance Health's ongoing commitment to responsible, high quality screening practices. The American College of Surgeons' Commission on Cancer (CoC) has designated Henry Ford Allegiance Health as an accredited cancer center. These distinctions are granted only to those facilities that have voluntarily committed to provide the best in cancer diagnosis and treatment and are able to comply with established CoC standards.
Planning and Development Process
Our Thoracic DST was established in 2009. This team includes physicians and leadership from the following areas: medical oncology, pathology, pulmonology, radiology, radiation oncology, and thoracic surgery. The team closely reviewed the literature on lung screening and was responsible for outlining the program standards, utilizing best practices and guidelines from the American College of Radiology (ACR), the Advisory Board, the Centers for Medicaid and Medicare (CMS), and the NCCN. A project management algorithm was completed outlining responsibilities and timelines for key tasks that needed to be implemented, including but not limited to process flow, qualifying criteria, costs, compliance, education, staffing, and marketing. A sub-committee of the Thoracic DST met offline to ensure progress through the work plan. This team included representatives from each area that would be impacted by the program. Buy-in from key stakeholders was relatively easy, as each area had a representative at the Thoracic DST/sub-committee meetings and had a voice in the decision-making process. Physician and staff education prior to the program launch was vital. Numerous multi-faceted educational efforts were deployed to ensure that stakeholders and staff throughout the system were informed on the vision, patient indications, and overall program goals. These included articles in the medical staff and employee newsletters, direct education to physicians and staff, huddles, and quality outcome reviews with the executive team and board of trustees. Following the launch of the lung-screening program, the Thoracic DST continued its responsibility to monitor quality measures and aid in resolution for areas of opportunity.
Description of the Quality Improvement Activity
Benchmarking for the quality indicators for the lung-screening program was determined by utilizing the ACR's National Radiology Data Registry (NRDR), NCCN Guidelines, and Medicare Local Coverage Determination criteria. A team comprised of members from multiple areas, including business management, finance, medical oncology, nursing, patient experience, quality, radiology, and radiation oncology worked to design and populate specific quality and finance metrics to include in the Thoracic Disease Site Team's overall balanced scorecard. This scorecard continues to be reviewed at every Thoracic DST meeting for continued monitoring of program financial vitality, patient satisfaction, quality, and learning and innovation. The areas tracked on the scorecard for the lung screening program include, but are not limited to, the following quality indicators:
- Lung screening appropriateness
- Lung rad category-total number, percent of the population, and percent at highest risk
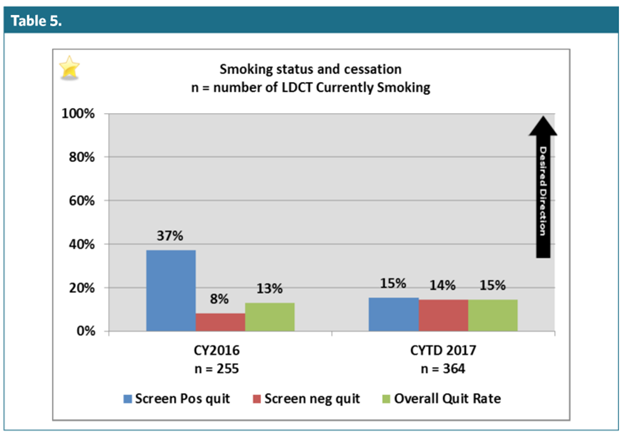
- Smoking status and cessation
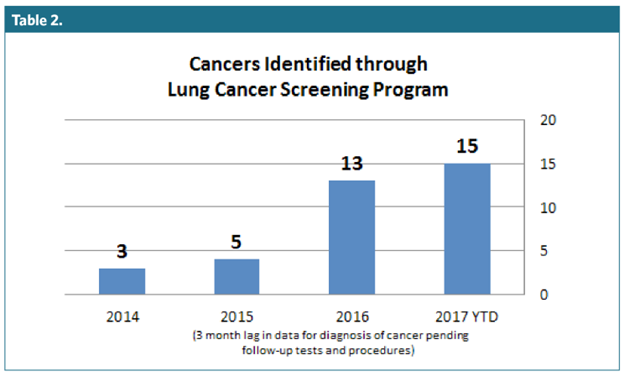
- Lung screening findings-tracking of incidental findings, lung cancer findings, and other cancer diagnosis findings
- Lung cancer detection rate
- Lung cancer stage at diagnosis-total number and percent
As areas of opportunity arise, the Thoracic DST provides guidance for action planning and monitors the progress. These items remain under review as long as the committee deems appropriate.
Resources Used and Skills Needed
Staff
Henry Ford Allegiance Health's Lung Cancer Screening Program is a patient-centered model. Our dedicated team includes a lung nodule navigator, dedicated radiologist, thoracic surgeon, tobacco cessation counselor, service line scheduler, and our radiology department. It was crucial to have the backing and support of the Thoracic DST in order to ensure engagement of all the areas impacted within and outside of the health system.
Costs
Investment in the dedicated support of a lung nodule navigator was a critical piece in the program's success. During the program's development phase, an oncology-certified nurse completed research and gathered best practices for the team's discussion. She also researched and implemented key regulatory and program components to ensure that the methodologies being deployed were based on sound generally acceptable practices.
Funding
Recognizing the passion of the Thoracic DST co-leadership and believing in the efficacy of the concept, the Jackson-based Tony Open Fundraiser generously donated $31,000 to Henry Ford Allegiance Health for the lung cancer-screening program in 2014. This support enabled our cancer program to provide 164 free screenings. On October 2, 2015, Medicare and private payors began covering low-dose lung screenings and a reimbursement model was adopted, causing the program to expand to meet a greater need in the community. In January 2017, Medicare decreased their payment by 46 percent; however, private commercial payors increased their reimbursement, leading to a sustainable program.
What Were the Results?
Since initiating the lung-screening program and as of December 31, 2017, there have been 1,228 screenings, resulting in a diagnosis of 36 cancers, 30 of which were lung cancer. The 2017 national lung cancer detection rate according to the Lung Cancer Screening Registry was 1.9 percent.* Our cumulative detection rate was 2.9 percent. Screening volumes have shown growth from 220 screenings in CY15 to 582 screenings in CY17. Henry Ford Allegiance Health has consistently met the lung screening appropriateness criteria based on a rigorous education of providers, a review process of referrals, and a user-friendly referral form and process. The Lung Rad Category 4 at screening has decreased from 67 percent in 2015 to 9.1 percent in 2017. Smoking cessation counseling at the time of screening has been an effective addition to our program. The quit rate for patients who had a negative screening has increased from 8 percent of patients in 2016 to 14 percent of patients in 2017. The overall quit rate for all screening patients also increased from 13 percent in 2016 to 15 percent in 2017. Program outreach resulted in the following distribution of physician referrals: 29 percent employed, 34 percent pulmonary clinic, and 37 percent independent in 2017. The overall downstream net revenue for 2016 was $3 million, suggesting that introduction to the system resulted in fuller health system loyalty.