The patient was later seen in our clinic for follow-up. She was doing well at that time, with minimal pain as well as denied nausea, vomiting, fevers, and chills. Her serum CA 19-9 had down trended to 51 units/mL at this visit. She followed up again a few weeks later in our clinic and continued to do well. Serum CA 19-9 had decreased further to 29 units/mL. Two months later, a CT A/P with contrast was completed due to a recurrence of right upper quadrant pain that showed postsurgical changes without any recurrence of or residual mass and no acute intraabdominal processes. Her pain was deemed likely musculoskeletal in nature given her recent return to work. The patient has not had any recurrent or new symptoms since that time.
Discussion
Serum carbohydrate associated antigen 19-9 is a well-known tumor marker of biliopancreatic malignancies. However, a number of benign pathologies are also associated with an elevated serum CA 19-9.1 While these elevations are typically mild (<200 u/ml), few etiologies, including obstructive jaundice, acute liver failure, acute hepatitis, alcoholic liver disease, and acute pancreatitis, have been known to cause more marked elevations (>1000 u/ml).1
Mucins carrying the CA 19-9 epitope are secreted by normal biliary cells.5 An elevated serum CA 19-9 indicates inflammation of the biliary tree or surrounding parenchyma with resultant biliary leakage into systemic circulation.5 The biliary epithelium that lines hepatic cyst walls has been proposed as the underlying etiology of elevated CA 19-9 in most benign cases.5 In cases of an infected cyst, these levels are even further elevated due to the local inflammatory state.5
Although using serum tumor marker CA 19-9 has been proposed as a diagnostic tool for differentiating malignant and premalignant lesions from benign cysts, studies have not supported this notion. Numerous studies have shown that neither serum nor cystic concentrations of CA 19-9 are reliable in differentiating hepatic cystadenomas and cystadenocarcinomas from simple hepatic cysts.2-4 However, the serum CA 19-9 derangements cited in these reports were much milder than that seen in our patient, all <200 u/mL. Despite the markedly elevated serum CA 19-9 of the patient, pathology was consistent with a benign hepatic cyst, further underscoring the poor predictive value of serum CA 19-9 in differentiating benign versus malignant biliopancreatic etiologies. Cyst aspirate was not obtained during this case and, thus, we are unable to further comment on cystic concentrations of CA 19-9 in this report.
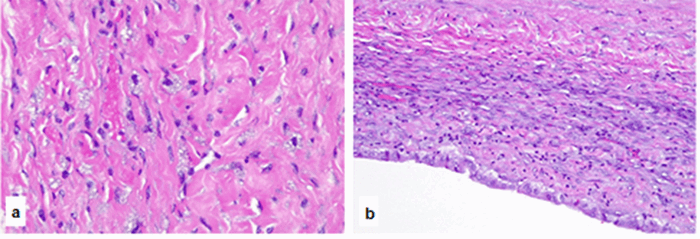
As described above, our patient’s mass was lacking a significant portion of the circumferential epithelial lining. The presence of numerous muciphages and occasional neutrophils and lymphocytes on pathology are indicative of a local inflammatory reaction leading to breakdown of the epithelial barrier surrounding the cyst. Breakdown of this epithelial lining would have allowed excess leakage of cyst contents (mucin) into the serum, leading to an elevated serum CA 19-9, as was seen in the patient’s lab results. There was also significant collagen and stromal tissue present at the periphery of the cyst, again indicative of a local inflammatory reaction.
Additionally, elevation of serum CA 19-9 in the setting of heavy black tea consumption has been observed. Al-Janabi and Tawfeeq6 described serum CA 19-9 elevation in 43 percent of subjects consuming large amounts of black tea. However, the maximum value observed among participants was 105 in this study. A 2003 case report described an individual with CA 19-9 levels elevated to >1,000 without any responsible etiology identified other than heavy tea consumption and, most notably, this value down-trended to normal limits with cessation of tea consumption.1 The patient endorses drinking several glasses of black tea on a daily basis.
While heavy consumption of black tea may have further contributed to or amplified our patient’s CA 19-9 elevation, it is likely that the histologic evidence of epithelial breakdown was primarily responsible for this patient’s markedly elevated serum CA 19-9 value of greater than 45,000, particularly given the significant decrease in value following surgical resection.
Conclusion
While serum CA 19-9 is a biomarker associated with biliopancreatic malignancy, it is also associated with a number of benign etiologies and cannot reliably be used to differentiate between the two. Our case report further supports the observation that serum CA 19-9 does not have value in predicting malignant versus benign etiology of biliopancreatic masses.
Lessons Learned
Although the case underscores the inaccuracy of serum CA 19-9 as a serological predictor of malignancy, the patient’s symptomatology in the presence of an enlarging hepatic mass was an appropriate indication for resection.
Authors
Williams LE; Chan EY; Pool MD; Thomas MB
Corresponding Author
Lauren Williams, MD
Department of Surgery
1750 W. Harrison St., Jelke-775
Chicago, IL 60612
Phone: (618) 919-1881
E-mail: lauren_e_williams@rush.edu
Author Affiliation
Rush Medical Center
Department of Surgery
Chicago, IL 60612
Disclosure Statement
The authors have no conflicts of interest to disclose.
References
- Howaizi M, Abboura M, Krespine C, Sbai-Idrissi MS, Marty O, Djabbari-Sobhani M. A new cause for CA19.9 elevation: heavy tea consumption. Gut. 2003;52(6):913-914. doi:10.1136/gut.52.6.913
- Park KH, Kim JS, Lee JH, et al. [Significances of serum level and immunohistochemical stain of CA19-9 in simple hepatic cysts and intrahepatic biliary cystic neoplasms.] Kor J Gastroenterol. 2006;47(1):52-58.
- Choi HK, Lee JK, Lee KH, et al. Differential diagnosis for intrahepatic biliary cystadenoma and hepatic simple cyst: significance of cystic fluid analysis and radiologic findings. J Clin Gastroenterol. 2010;44(4):289-293. doi:10.1097/MCG.0b013e3181b5c789
- Yanai H, Tada N. A simple hepatic cyst with elevated serum and cyst fluid CA19-9 levels: a case report. J Med Case Rep. 2008;2:329. Published 2008 Oct 14. doi:10.1186/1752-1947-2-329
- Kanaan N, Goffin E, Pirson Y, Devuyst O, Hassoun Z. Carbohydrate antigen 19-9 as a diagnostic marker for hepatic cyst infection in autosomal dominant polycystic kidney disease. Am J Kidney Dis. 2010;55(5):916-922. doi:10.1053/j.ajkd.2009.12.023
- Al-Janabi AAHS, Tawfeeq EF. Interfering Effect of Black Tea Consumption on Diagnosis of Pancreatic Cancer by CA 19-9. J Gastrointest Cancer. 2017;48(2):148-150. doi:10.1007/s12029-016-9855-z