Become a member and receive career-enhancing benefits
Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
Become a member and receive career-enhancing benefits
Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
Surgeons Handle New and Alarming Pathology—Xylazine Wounds
M. Sophia Newman, MPH
October 1, 2025
15 MinPrintShare
Bookmark
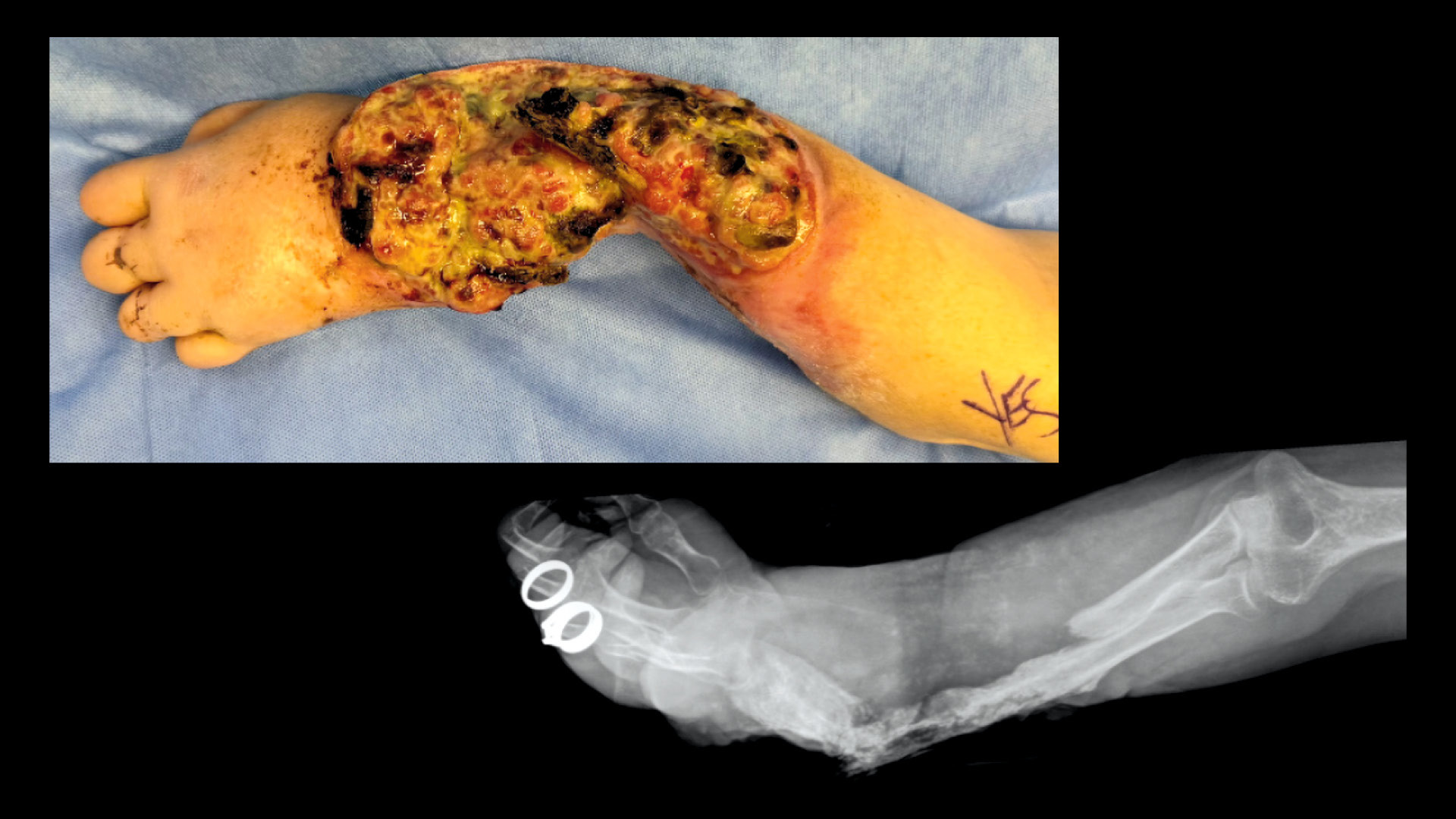
This photograph and radiographic image show a forearm with severe xylazine wounds and related osteomyelitis and bone fracture.
Over the past 2 decades, the US opioid epidemic has resulted in the deaths of 727,000 individuals by overdose alone1— and in recent years, a startling new complication of opioid use has emerged.
Initially fueled by clinicians’ overprescription of opioid medications, the epidemic has long since shifted into a three-pronged mix of prescription opioids, heroin, and hyper-potent synthetic opioids, most notably fentanyl. Synthetic opioids now constitute much of the illicit drug supply and cause the largest share of overdose deaths.1
Additionally, fentanyl and similar drugs are often contaminated with a range of other drugs. One particularly harmful contaminant, xylazine, presents a new medical issue that surgeons in many disciplines need to understand: severe, necrotic wounds that can cause amputations and even mimic necrotizing fasciitis.
As a result, numerous clinicians in hard-hit cities are engaged in efforts to understand, effectively treat, and educate surgeons and others on this new pathology.2-4 Asif Ilyas, MD, MBA, FACS, an orthopaedic surgeon and opioid use researcher at Rothman Orthopaedics and Drexel University, both in Philadelphia, Pennsylvania, said, “I look at it as a new chapter of the opioid crisis.”
These xylazine wounds on the forearms are of moderate intensity.
For Lisa Rae, MD, FACS, chief of burn surgery at Lewis Katz School of Medicine at Temple University in Philadelphia, Pennsylvania, a patient arrived with an injury that looked like a radiator burn. This patient, who had active opioid use disorder, presented with deep, elongated wounds on his back—an impossible spot to inject drugs. She assumed the stripes came from a contact burn from a hot radiator, a cause the man denied. Only after the same man appeared again with similar wounds in late spring, followed by a second such patient, did she understand that the cause lay elsewhere. These wounds were a particular variation on the extreme problem that xylazine causes.
After the α2-adrenergic receptor agonist drug was first synthesized in 1962, research into human use was discontinued upon the discovery of its tendency to create severe necrotic wounds in users.
Because this result does not occur in nonhuman mammals, xylazine entered manufacture as a veterinary sedative only. Decades later, illicit use began in Puerto Rico, where some users sought the intense sedation the drug creates. Nicknamed “tranq,” the drug spread, emerging around 2015 as a contaminant of the illicit fentanyl supply in the continental US.
In Philadelphia, a city known for the intensity of its opioid crisis, street-sold opioids began showing high rates of contamination several years ago; from January through May 2024, for instance, virtually all tested samples in the city included xylazine.5 A substantial part of the fentanyl supply nationwide is now contaminated with this drug.6
The result is a population of patients with dramatic and often complicated wounds. Interestingly, the wounds can occur at both injection sites and distant locations across the body—as with the patients Dr. Rae saw with wounds on their backs.
This image shows severe wounds with exposed and crumbling bone.
Although the full pathology is not yet clear, Dr. Ilyas noted early insights on local wounds: “The thought is that xylazine is likely causing these wounds by one of a couple potential mechanisms. One is, it’s causing a local tissue toxicity—almost like a burn. The second is that it is causing some local vasoconstriction, reducing blood flow and oxygen to the area. The combination of these potential mechanisms is lending itself to these wounds that, with repetitive injecting, gets worse and worse and worse.”
The result is a startling spectrum of severity. Dr. Ilyas explained, “We’re seeing mild cases with early wounds forming, and we’re seeing other folks who have been injecting for such a long time that their limbs have become mummified.”
In other words, these wounds are so deep they expose tendons and bones, which then become so damaged by osteomyelitis that they sometimes spontaneously crumble.
Dr. Rae concurred that cases are often severe.
“We have people who have eroded tissue through their chest wall. Their lung is out. We’ve seen the innominate artery. One woman had fistulas and opened up her entire abdomen. Never mind the bones and the maggots and the smell,” she said.
The range of presentations includes milder cases that involve areas of reddened and blackened tissue. Although wounds can occur on most body parts, many are on limbs, particularly forearms, the most frequent sites of injections.
Wounds may vary by location, according to Dr. Rae. At injection sites, they present first as small abscesses with blisters, then larger wounds that are purple and ischemic. In contrast, distant sites tend to involve deep, oblong wounds with areas of frank necrosis.
At times, Dr. Rae explained, both types may resemble vasculitis or even necrotizing soft tissue infection (NSTI), which is also known as necrotizing fasciitis.
For a wide range of surgeons, including those in general, trauma, and acute and critical care surgery, this may be how they first encounter xylazine wounds: during a consultation for possible NSTI, a situation that can call for a rapid trip to the OR for radical excision of diseased tissue and a high chance of amputation—with the alternative being nearly guaranteed, often rapid mortality.
Avoidable Amputations, Unworkable Skin Grafts, and Delayed Osteomyelitis Care
But xylazine wounds are not necrotizing fasciitis. Indeed, in some ways they are quite far from it.
For consulting surgeons, the first thing to note is the differences in the symptom picture. Patients with xylazine wounds typically have pain proportionate to the severity of their wounds, low-grade or no fever, normal vital signs, normal blood counts, and a small abscess or unremarkable findings on computed tomography scans.
In contrast, a patient with NSTI will present with extreme pain, high fever, an elevated white blood cell level, a rapid heartbeat and respirations, hypotension, abscess and/or soft tissue gas on computed tomography, and a range of possible late signs, including sepsis. While both patient groups may present with nausea, vomiting, and diarrhea, patients with xylazine wounds will have those symptoms only because of drug withdrawal, while patients with NSTI experience them as part of the fulminating infection (see Table).
Table. Xylazine Wounds Versus Necrotizing Fasciitis
Perhaps most importantly, the urgency and potential outcomes of xylazine wounds are far milder than those of NSTI. “These aren’t life-threatening. They’re limb-threatening, but not life-threatening,” Dr. Ilyas explained.
While the mortality rate for untreated NSTI is extremely high, patients with xylazine wounds—even those who are totally noncompliant with care—almost always survive.
About her own experience in clinic, Dr. Rae said: “We’re seeing just this purple, horrible, necrotic tissue, and I’m just talking doctors off a ledge and going, ‘No, no, we know what this is. They’re okay, I promise. I’ll monitor them closely. They don’t need to be rushed to the OR and have a radical excision of all their skin. Let them demarcate and heal, and we’ll do wound care and things like that.’”
The treatment process for xylazine patients is often surprisingly simple, involving nonaggressive wound debridement, a dermal substitute to cover the wound, and watchful waiting. By the accounts of Drs. Rae and Ilyas, as well as published accounts from other clinicians and patients, the affected people who manage to cease using xylazine-contaminated drugs often heal well with no further interventions.
In many cases, this can be enough to mitigate the threat to the limb. While some xylazine wounds do lead to amputation—an investigation by The Philadelphia Inquirer7 found that, in that city, amputations among people addicted to opioids doubled between 2019 and 2024—clinicians now understand that xylazine wounds tend to heal better than most other wounds of similar size, depth, and severity. This is true even for injuries that could require an amputation if they arose via other causes.
In fact, a similar wound from a non-NSTI cause might require a skin graft, with patients unable to epithelialize the wound and heal fully without one.
Although the underlying biology is not yet determined, Dr. Rae posited that the very method by which drug users accumulate harm also marshals resources for faster and more complete healing.
“They have a chronic wound cycle where they keep injecting and their body’s trying to heal, so they actually have all the healing mechanisms in that wound when we take out the dead tissue, and we try to take out as little as possible. They grow new tissue and heal into it very, very quickly, much more quickly than I see in a healthy burn patient who has tissue necrosis, because all those elements need to make their way into the wound,” she said.
For patients with xylazine wounds, she advised against skin grafting. She noted that ongoing injections of street drugs at or near the site can destroy a graft. Additionally, creating a tissue donor site introduces both a site for xylazine wound recidivism and additional care needs—a challenge to a patient population who are often unhoused and/or lacking access to appropriate sanitation and hygiene supplies.
“I employ a harm reduction strategy rather than a curative one. Dermal substitutes can help patients heal or grow tissue to protect exposed bone and tendon without definitive wound closure while they are still injecting. Graft and donor sites are high risk at this stage, and we find many patients heal without needing a skin graft over the dermal substitute,” Dr. Rae explained.
For patients with tissue damage that is exposing bone, the lack of skin coverage can lead to chronic osteomyelitis. Although consensus is not universal, the general wisdom is that treating these bone infections is best delayed until wound closure has been attained.
“You can manage both the skin wounds and the osteomyelitis simultaneously,” Dr. Ilyas said.
He also noted that treating these infections is often delayed until closure of open skin, which can help ensure maximal benefit. “We’re not being as aggressive with the osteomyelitis because we need soft tissue coverage if the bone infection is to resolve.”
Patient-Centered Care
Dr. Rae acknowledged that this careful, slow-moving strategy can feel inconsistent with the decisive, curative approach to which many surgeons are accustomed. What she and others have raised is the strong need for patient-centered care,8 including a willingness to engage with patients who do not fully cease drug use.
“We’ve changed our paradigm to be less aggressive surgically for these wounds and really base our surgical intervention on the stage of the wound and then the patient’s compliance with substance abuse treatment,” Dr. Ilyas said, because the level of healing is so often contingent on drug cessation.
To that end, physicians also are increasingly engaged in ensuring that patients have adequate access to both addiction medicine and pain management specialists while undergoing wound care. This approach helps reduce a common problem among affected patients: the combined withdrawal of xylazine and opioids can be so challenging to tolerate that the rate of xylazine-affected patients leaving the hospital against medical advice has increased to roughly half of all inpatients.7
As a result, treatment can include opioid drugs—an often-uncomfortable experience for surgeons who are reluctant to prescribe the large doses these patients have come to tolerate—as well as methadone, buprenorphine, clonazepam, and other drugs meant to assuage withdrawal symptoms and the pain associated with xylazine wounds.
For Dr. Rae, prescribing large doses of opioid drugs has been a learning experience for herself and other hospital staff members.
“There’s a lot of misunderstanding that they’re just, you know, having fun and using it,” she said. “But there is nothing you could give them that causes euphoria anymore. That chase is over. They’re just stuck in a cycle of not feeling well.”
The result of clinician misperception can be the unwitting withholding of necessary medications and an experience of rapid withdrawal that intensely sickens and distresses the patient. After appropriate treatment for withdrawal upon admission and a few days of titration of medication for ongoing symptoms, a healthier and calmer patient can emerge.
“Patients are simply sick from withdrawal,” Dr. Rae said. “When we fail to treat the withdrawal symptoms so that they cannot stay in the hospital to receive the care they came for, it’s our fault as doctors.”
Consensus Statements and Standards
A decade after xylazine began contaminating illicit opioids, physicians are attaining consensus on how to best treat the resulting wounds.
In November 2024, Dr. Ilyas’s nonprofit research organization, the Rothman Institute Foundation for Opioid Research & Education, held a symposium on the xylazine crisis in Pennsylvania at the Sidney Kimmel Medical College in Philadelphia. The event generated a consensus statement2 that offers a classification system for xylazine wounds (see sidebar), an algorithm for understanding when amputation may be necessary, and extensive insight into wound care, pain management, social services, ethical considerations, and policy goals.
In April 2025, the University of Pittsburgh Medical Center (UPMC) in Pennsylvania announced it was among the first health systems to implement standards procedures for treating xylazine wounds. As with the Philadelphia group, they convened clinicians from numerous specialties to understand how to balance wound care with withdrawal management strategies and addiction medicine.4
Temple University, Dr. Rae’s institution, also is working on a publication on treatment protocols that similarly engages a wide range of clinicians into helping ensure optimal care to patients.
The forearm and hand exhibit moderate xylazine wounds.
Vision of Hope
Amid the ongoing crisis, there is good news: the presence of xylazine in illicit fentanyl appears to be dropping, per the Philadelphia Department of Public Health. Although virtually all fentanyl tested contained xylazine in May 2024, by December, that rate was 42%.5
Additional opioid additives, including medetomidine and nitazines, are now contaminants of concern. But to date, none of these appears to be associated with the severe tissue injuries that xylazine causes. (Medetomidine, which is among the most frequently encountered additives, causes somewhat alarming but largely nonharmful bradycardia.)
Researchers and clinicians have identified many steps that are helpful for the optimization of care, including a xylazine wound-specific code for hospital records, to help facilitate research and follow-up; state and federal policies, particularly ones making xylazine a controlled substance; and ongoing clinician education. For now, progress toward care protocols can help raise hope among drug users, the healthcare personnel who serve them, and the communities impacted by the opioid crisis.
It also may engage surgeons and other clinicians in what may be a once-in-a-lifetime clinical experience. As Dr. Rae noted, “We don’t see a lot of new pathology come our way in medical science. To have something new to figure out from a surgical standpoint is a very interesting moment.”
M. Sophia Newman is the Medical Writer and Speechwriter in the ACS Division of Integrated Communications in Chicago, IL.
Ilyas AM, Ramtin S, Ilyas EN, et al. Philadelphia consensus on the surgical management of xylazine-associated wounds in people who use drugs. SurgiColl. 2025;3(2).
Tosti R, Hozack BA, Tulipan JE, Criner-Woozley KT, Ilyas AM. Xylazine-Associated wounds of the upper extremity: Evaluation and algorithmic surgical strategy. Journal of Hand Surgery Global Online. 2024;6:605e609.
Shang M, Hull I, Liebschutz JM, et al. Building multidisciplinary consensus on inpatient xylazine management through clinical protocols. Subst Use Addctn J. 2025 Apr 15:29767342251329681.
Philadelphia Department of Public Health Division of Substance Use Prevention and Harm Reduction. Health Alert: Hospitals and behavioral health providers are reporting severe and worsening presentations of withdrawal among people who use drugs (PWUD) in Philadelphia. Published December 10, 2024. https://hip.phila.gov/document/4874/PDPH-HAN-00444A-12-10-2024.pdf/. Accessed July 1, 2025.
Butler Center for Research. Research update: Harm reduction: History and context. Published January 2023. https://www.hazeldenbettyford.org/research-studies/addiction-research/harm-reduction. Accessed August 8, 2025.