Robotic endoscopic ports are used for mitral valve repair at UChicago Medicine.
“During my residency in the early 1990s, the big conversation was ‘Do we need to teach residents how to do open gallbladder resection before we switch over to laparoscopic cholecystectomy?’ That’s not a conversation anymore—it’s a given that the gallbladder will be taken out with a scope, and the residents will learn how to do it that way,” said Dr. Balkhy. “We’re not there, obviously, in cardiac surgery, but we now see that residents know how the robot works. They know how to operate the arms and the pedals, and they understand the robotic environment. So even though we continue to train them in the open setting, getting them transitioned to the robot is a much easier endeavor.”
While robotic skills training is largely absent from cardiac surgical residency training, more institutions are bringing robotic cases into their programs. Notably, the majority of US cardiac surgeons must complete a general surgery residency program—where training in robotics is increasingly an area of focus—before specializing in cardiothoracic surgery.
“We have residents in the middle of their general surgery training coming in and doing rotations with us in the robotic room, and they’ll be able to do parts of the operation very easily,” explained Dr. Balkhy. “When I first started doing robotics and was 10 years into my practice, it was not that easy because we did not have that training as residents.”
In the OR during the world’s first robotic lung transplant, the primary surgeon sits at a console that is connected to the robot at the bedside.
Associated Risks and Outcomes Data
“The risks of robotic cardiac surgery are very similar to risks associated with the same procedure in a standard approach,” said Dr. Emerson. “The concern we have that is more specific to the robot is the need for conversion. If you’re in any kind of minimally invasive approach and you have to urgently change what you’re doing and get larger access, obviously that’s an additional step, where in a case that’s already open, you’re right there and you can deal with it more expeditiously.”
In a review of articles published between 2015 and 2023, researchers validated the “dependability” of robotic-assisted cardiac surgery with “encouraging” outcomes that demonstrated shorter operating times, reduced blood loss, and a low incident of conversion to conventional interventions.4 The mortality rates overall were shown to be similar between robotic and traditional cardiac surgery.
“The top cardiac approaches done with the robot are mitral valve and CABG,” Dr. Emerson said. “The data indicate that, especially in larger centers with higher volume, you are not in any way sacrificing outcomes. Your outcomes are at least as good as the traditional approaches in select populations. Yes, there are conversion rates—there are times that you have to say ‘Okay, well, I need to bail on the robot. I’m going to go to a full thoracotomy or I’m going to do a sternotomy.’ But those rates are generally low, and they decrease over time with experience.”
A study coauthored by Dr. Balkhy and published in a 2025 issue of The Annals of Thoracic Surgery examined 550 robotic totally endoscopic mitral valve surgeries.5 The 30-day surgical success rate was 95.9%, and procedural success was 93%. “Postoperative echocardiography revealed no or trace residual mitral regurgitation (MR) in 95% and mild residual MR in 5%,” noted the study authors.
“Our mitral valve experience had a 95%, 5-year freedom from reoperation for recurrent MR,” added Dr. Balkhy. “But one of the key takeaways here is to focus on robotics as a matter of routine, so that the device doesn’t become a nuance every time you enter the OR, but instead, it is a natural part of the room. If I walk into my room any day of the week and I don’t see a robot—I’m lost. Where’s my robot?”
Robotic cardiac surgery requires thoughtful setup of the machine to ensure adequate room to maneuver within the chest. Dr. Dominic Emerson prepares the robot for a mitral valve repair.
Innovations in Robotic-Assisted Cardiac Surgery
Before describing advancements in robotic-assisted cardiac surgery, it is important to understand that the surgeon remains in control of the entire operation. However—as a recent procedure conducted at Johns Hopkins University in Baltimore, Maryland, revealed—that reality may be changing in the future.
“I’m sure a common question faced by every robotic surgeon is ‘Who is conducting the procedure—the surgeon or the robot?’,” said Dr. Emerson. “I think patients sometimes wonder if I’m just standing off to the side having coffee while the robot is doing the surgery—and the answer is, obviously, ‘No.’ I tell patients that the robot is simply an extension of me. However, the future is probably going to be different. I believe that at some point there likely will be some independence for the robot—just look at what the group at Hopkins recently accomplished.”
In July 2025, an artificial intelligence (AI) system trained on 17 hours of video depicting Johns Hopkins surgeons performing gallbladder removals on pig cadavers.6 With almost no human intervention, the AI-driven robot separated the gallbladder from the liver in a dead pig, in an event that researchers suggest is the first realistic surgery conducted autonomously by a machine.
“I think AI or machine learning is going to have an impact on cardiac surgery just like it will with every other aspect of medicine,” Dr. Emerson said. “I think it will probably manifest most quickly in things like data analysis, which could help us become more efficient in the operation. I also believe there will be continued integration of other technologies, such as imaging analysis and the ability to see overlays of structures in real time.”
Dr. Balkhy supports the conclusions drawn by Dr. Emerson regarding wide-scale adoption of independent robotic surgery.
“I am usually on the cutting edge of things and trying to adopt the latest and greatest, but I’m also extremely conservative when it comes to safety,” explained Dr. Balkhy. “I think the systems are not refined enough yet, especially in cardiac surgery. Pretty much all my coronary bypass procedures are on the beating heart—so things are moving, the lungs are moving. Now, it’s not that AI can’t account for that. It probably can. We have very smart engineers and smart systems that can do that, but the safety bar is extremely high.”
Before autonomous robotic surgery can move forward, the technology needs to master small, simple tasks. During CABG, for example, when a healthy blood vessel is used to bypass a blocked coronary artery, surgeons need to harvest a vein or in the case of robotic coronary surgery an artery—a task parts of which a robotic device potentially could complete independently.
“This sequence of events, which takes about 30 to 45 seconds between instrument exchanges, could potentially be automated such that there is a self-reloading clip that goes in and it changes into a cutting instrument all within 10 seconds,” said Dr. Balkhy. “It seems to me that a simple thing like that, as long as it’s well controlled and there is not a risk of injury, could be done autonomously with a robot—but we’re not there yet.”
While autonomous surgery remains a future prospect, other innovations in robotic-assisted cardiac surgery are already underway, including applications in transplantation and telesurgery.
In 2021, surgeons at Cedars-Sinai Medical Center performed the world’s first robotic-assisted lung transplant. Using the robotic platform for the donor-to-recipient anastamoses, a 69-year-old patient received a new right lung.
“We believe robotic-assisted surgery is the future of lung transplantation,” said Dr. Emerson, the lead surgeon, in a press release.7 “We have transitioned from offering traditional lung transplantation to minimally invasive lung transplantation to now, robotic-assisted capabilities. This long-awaited achievement is the start of a new era of cardiothoracic care.”
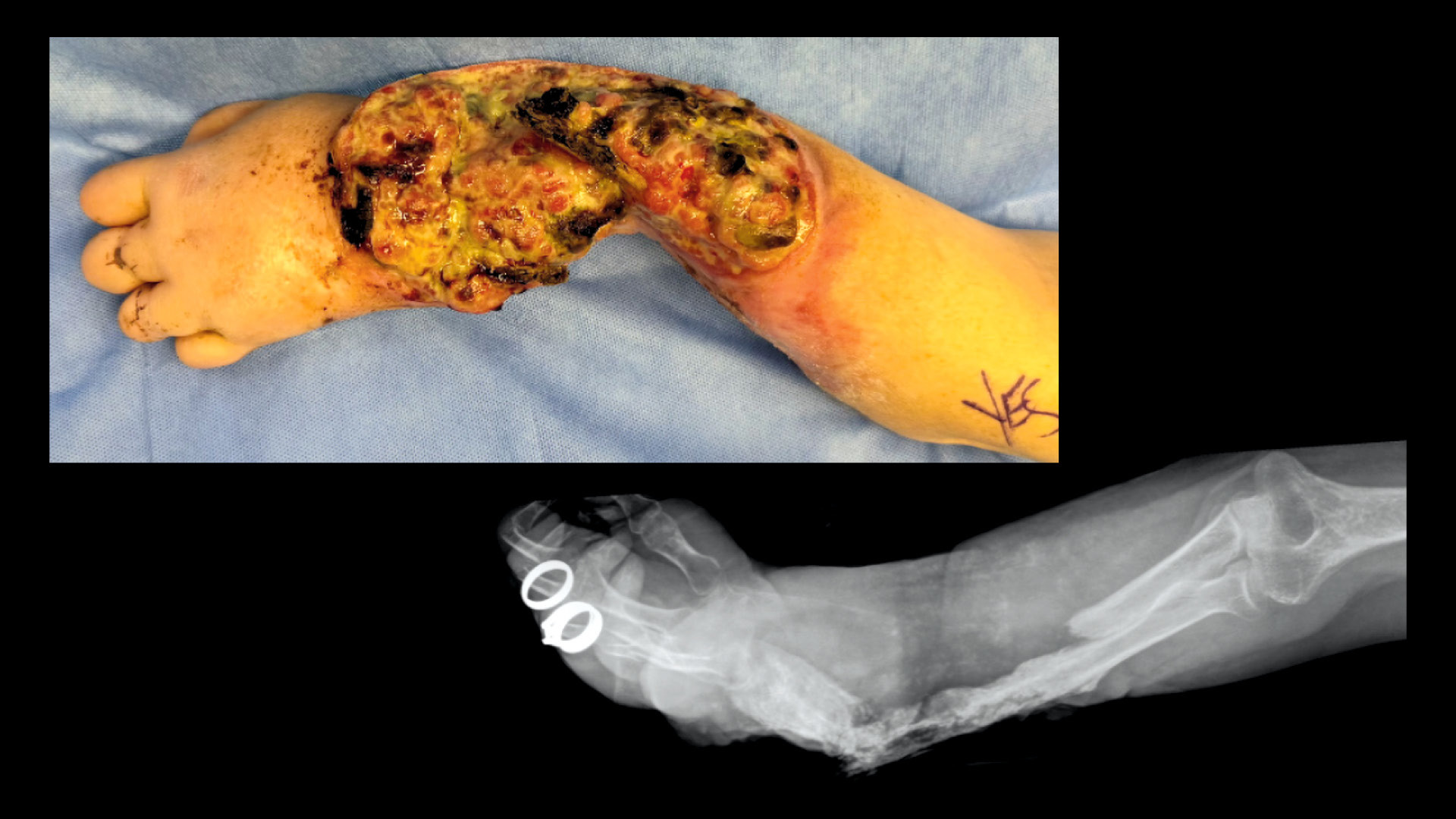
Using the robot, transplant surgeons can perform a lung transplant through incisions as small as 5-6cm. Here, the new donor lung is shown alongside the incision used to perform the operation.
The team at Cedars-Sinai initiated the use of smaller incisions “no larger than the short side of a driver’s license” that resulted in reduced postoperative pain and improved recovery for the patient.
Robotic-assisted advancements in transplantation also include the world’s first fully robotic double lung transplant in 2024 at New York University Langone in New York, and the first robotic heart transplant in the US performed by surgeons in 2025 at Baylor St. Luke’s Medical Center in Houston, Texas.
Another emerging area in robotic cardiac surgery is telesurgery and its ability to expand access to advanced surgical care over great distances. Earlier this year, Dr. Balkhy moderated what is considered to be the world’s first intercontinental robotic cardiac telesurgery.8 The procedure, an atrial septal defect closure, was conducted remotely from a facility in Strasbourg, France, to an OR in Indore, India.
“A lot of these new robotic systems have really jumped into telesurgery, and that’s happening through both fiber cables and through 5G,” said Dr. Balkhy. “This is exciting because, initially, robotic surgery was focused only on the first world, and now this specialized care can be offered to patients in low- and middle-income countries. Imagine a world where a person can go a short distance, maybe a half an hour away instead of 5 hours and have a blood clot taken care of by an expert living in a main city.”
Cardiac surgery will continue to evolve with safer, less invasive, and more efficient interventions that will improve the quality of life for heart patients everywhere.
“The sky’s the limit—it really is,” said Dr. Emerson. “Ten years ago, if you had said that we’re going to use the robot in the valve, people would have thought you were crazy. Five years ago, nobody had done a solid organ transplant in the chest with the robot. Robotics are going to continue to be an essential part of the cardiac surgery armamentarium. Our trainees want to learn it, our patients are asking for it, and our referring physicians want it.”
Tony Peregrin is Managing Editor, Special Projects, in the ACS Division of Integrated Communications in Chicago, IL.
References
- Bonatti J. Historical landmarks in the development of robotic coronary bypass grafting. Ann Cardiothorac Surg. 2024;13(4):332-338.
- Patrick WL, Iyengar A, Han JJ, Mays JC, et al. The learning curve of robotic coronary arterial bypass surgery: A report from the STS database. J Card Surg. 2021;36(11):4178-4186.
- Lin CY, Liu YC, Chen MC. et al. Learning curve and surgical outcome of robotic assisted colorectal surgery with ERAS program. Sci Rep. 2022. Available at: https://www.nature.com/articles/s41598-022-24665-w#:~:text=There%20are%20three%20stages%20of,system6%2C7%2C8. Accessed August 5, 2025.
- Fida Z, Ghutai G, Jamil Z, Dalvi AA, Hassaan M, Khalid K, Ali UA, Sivadasan M, Limbu K, Anthony N, Chaudhary JH, Ijaz MH, Pervaiz S. The role of robotics in cardiac surgery: Innovations, outcomes, and future prospects. Cureus. 2024;16(11):e74884.
- Kitahara H, Nisivaco S, Bhasin R, Hamzat I, et al. 550 robotic totally endoscopic mitral valve surgeries within a comprehensive robotic cardiac program. Ann Thorac Surg. 2025;119(6):1270-1277.
- Walker-Stokel C. Surgical robots take step towards fully autonomous operations. New Scientist. July 9, 2025. Available at: https://www.newscientist.com/article/2487575-surgical-robots-take-step-towards-fully-autonomous-operations/. Accessed August 5, 2025.
- Cedars-Sinai. Surgeons complete robotic-assisted lung transplant. Press release. January 28, 2022. Available at: https://www.cedars-sinai.org/newsroom/in-a-first-surgeons-complete-robotic-assisted-lung-transplant/. Accessed August 5, 2025.
- Surgical Robotics Technology. SS Innovations completes world’s first intercontinental robotic cardiac telesurgery. July 22, 2025. Available at: https://www.surgicalroboticstechnology.com/news/ss-innovations-completes-worlds-first-intercontinental-robotic-cardiac-telesurgery/. Accessed August 5, 2025.