After years of decline driven by successful tobacco cessation efforts, certain head and neck cancers—particularly oropharyngeal cancers—are on the rise in the US, largely due to increasing rates of infection with high-risk strains of human papillomavirus (HPV).
“The traditional cancers associated with tobacco consumption, such as mouth, tongue, and larynx cancer, have decreased,” said Dennis H. Kraus, MD, FACS, ACS Second Vice-President. “But other cancers, especially those related to HPV, are increasing significantly.”
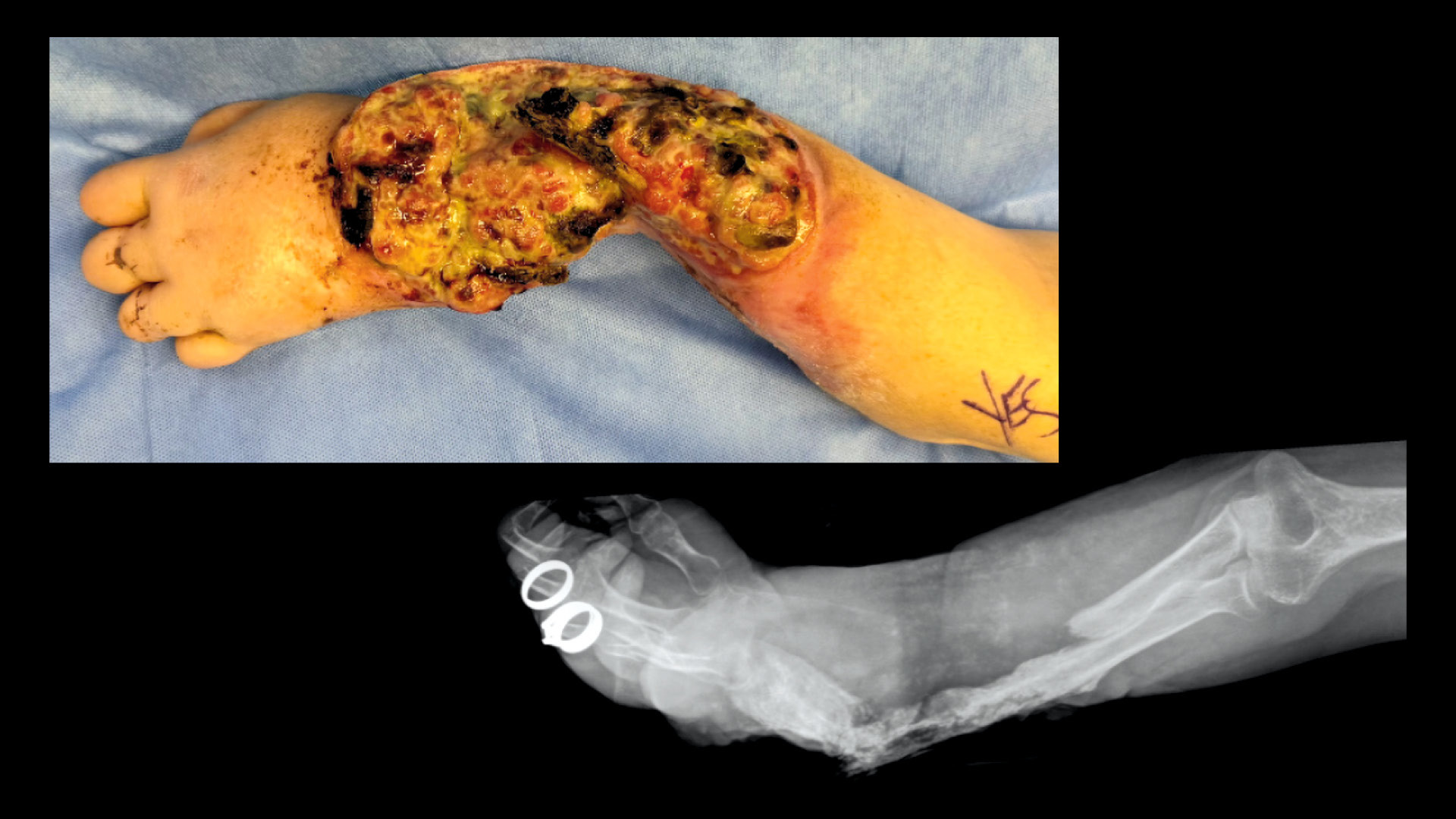
Head and neck cancers are a diverse, challenging disease group because they are near vital organs and complex in nature, and their treatments have the potential for significant side effects. The tumors’ proximity to structures like the larynx, salivary glands, and nerves can make it difficult to effectively target cancer cells without damaging healthy tissue.
Despite its morbidity, open surgery was once the mainstay of treatment for head and neck cancer, Dr. Kraus said. Then radiation and chemotherapy showed effectiveness but came with toxic side effects.
In recent years, minimally invasive surgical techniques and robotic-assisted surgery have been shown to treat head and neck cancers with less morbidity. Meanwhile, efforts to make radiation and chemotherapy more effective and less toxic are advancing, as are promising new developments in immunotherapy.
Since these treatments often are used in combination, effectively treating, reconstructing, and rehabilitating the head and neck cancer patient requires a multidisciplinary team.
Evolving Nature, Risk Factors
Head and neck cancers usually begin in the squamous cells that line the mucosal surfaces of the head and neck, or, less commonly, in the salivary glands, sinuses, or muscles and nerves in the head and neck.1 Other head and neck cancers include skin cancer and thyroid cancer.2
“Head and neck cancer is not one single cancer, it’s a constituency of diseases,” Dr. Kraus said.
The National Cancer Institute estimates that approximately 72,680 people in the US will be diagnosed with a major type of head and neck cancer—oral cavity, pharynx, or larynx cancer—in 2025. An estimated 16,680 people will die from these diseases.3
Most head and neck cancers can be divided into two different categories—those related to HPV and those that are not, said Jamie A. Ku, MD, FACS, director of the Head and Neck Robotic Surgery Program at the Cleveland Clinic in Ohio.
Historically, most head and neck cancers in the US were caused by tobacco use, often combined with alcohol use, and typically affected men 50 years and older.
Currently, though, HPV-driven cancers represent a large proportion of new head and neck cancer diagnoses in the US, which occur more commonly in men who are in their 40s or older, but also in women, said Ryan J. Li, MD, MBA, FACS, professor and chief of the Division of Head and Neck Surgery at Oregon Health & Science University in Portland.
“These patients are younger, healthier, and usually nonsmokers. They also have a slightly higher socioeconomic and educational background,” Dr. Ku said.
Tobacco-related head and neck cancers, however, are still prevalent in much of the world and are the third-most prevalent cancer, according to the Global Cancer Statistics of 2020. These diseases account for 7.6% of all cancers, 4.8% of all cancer-related deaths, and are predicted to rise 30% annually until 2030.4,5
“In Southeast Asia and India, oral cancer related to tobacco use and betel nut chewing is a major epidemic,” Dr. Li said.
Other risk factors include alcohol, environmental and occupational exposures (such as wood dust and mining), and genetic predisposition.
HPV Leads to Cancer Resurgence
HPV is the most common sexually transmitted infection in the world. Although most people resolve HPV infection without medical intervention, HPV-driven head and neck cancer can remain latent, grow slowly, and may not appear for years.6 In the US, head and neck cancers now surpass cervical cancer as the most common HPV-related malignancy, in part due to the success of cervical cancer screening.7
The rise in HPV-driven head and neck cancers in the US may be in part due to substantial differences in sexual practices in North America, Dr. Li said. The number of oral sex partners is a risk factor associated with HPV-related head and neck cancer, specifically oropharyngeal cancer.
HPV cancers have risen despite the introduction of the HPV vaccine in 2006 for girls and young women, and a few years later, for boys and young men. The most recent vaccine protects against nine high-risk HPV variants and is typically offered to patients upon their sexual debut up to the age of 26, but clinicians and patients can consider vaccination up to age 45 years, Dr. Li explained.
According to Dr. Ku, it may take 20 to 30 years before the HPV vaccine starts to reduce HPV-driven head and neck cancers.
Multidisciplinary Team Approach
Multidisciplinary collaboration is important when developing a patient plan that considers the roles of surgery, radiation, and systemic therapy, Dr. Li said.
The team typically includes surgeons, particularly otolaryngologists and head and neck, maxillofacial, and reconstructive specialists. At some US centers and around the world, this team includes general surgeons who subspecialize in head and neck cancer surgery, Dr. Li explained. In addition, many other specialists engage in treatment, reconstruction, and rehabilitation of these patients, including pathologists, radiologists, radiation and medical oncologists, speech and language pathologists, dentists, and nutritionists.
“Multidisciplinary care, especially for these complex head and neck cancer patients, is very important,” Dr. Ku said. “Patients should not be seeing just a surgeon. They should be under the care of a well-run team of specialists.”
“High-Risk Real Estate”
Cancer in the head and neck area can affect a patient’s appearance and sense of identity, as well as their ability to speak, swallow, and interact with others.
“The head and neck are very high-risk real estate,” Dr. Ku shared.
Minimally invasive and reconstructive techniques are critical to protecting patient quality of life. As a result, treatment decisions must take into account not just effectiveness in treating the cancer but also potential side effects—both short and long term. Radiation toxicity, for example, can potentially create quality-of-life issues, especially around swallowing and speech functions and dental and oral cavity health.
“That’s why patient selection is such a critical art and why surgeons must help patients understand the advantages and disadvantages of each approach,” Dr. Li said.
The effects of toxic radiation have become a rising concern in the US as HPV-driven cancers have become the most common cause of head and neck cancer.
HPV-related head and neck cancers, which primarily occur in the oropharynx behind the oral cavity, have a higher probability of cure than the classic head and neck cancer diagnosis that was related to tobacco use, Dr. Li said, adding that the longer the patient lives after treatment, the more likely the cumulative effects and toxicity of radiation can affect them post-treatment.
“They have a longer runway of time to experience adverse effects,” he said.