Become a member and receive career-enhancing benefits
Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
Become a member and receive career-enhancing benefits
Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
Civilian Surgeons Helped Shape Casualty Care in World War II
Danielle B. Holt, MD, MSS, FACS, and Jeremy W. Cannon, MD, SM, FACS
October 1, 2025
7 MinPrintShare
Bookmark
Collaboration between civilian and military surgeons has long accelerated surgical innovation. In World War II (WWII), the US Army embraced this synergistic approach by commissioning experienced civilian surgeons as consultants. Amid intense fighting and high casualty numbers, these consultants promoted a culture of practice improvement and disseminated lessons learned. After the war, the surgeons continued to spread their hard-earned knowledge through academic society meetings and written histories.
Foundations of the Consultant System
At the beginning of WWII, the US War Department’s medical system was under-resourced for a large-scale conflict having dramatically downsized after World War I (WWI). Brigadier General Fred Rankin, MD, FACS, a highly regarded general surgeon and WWI veteran, brought together leading civilian academic surgeons—including Edward (“Pete”) D. Churchill, MD, FACS, and Elliott Cutler, MD, both of Harvard Medical School, and Ashley W. Oughterson, MD, of Yale University—into the newly formed Surgical Consultants Division within the Army Surgeon General’s office.1-3 As described in Dr. Churchill’s Surgeon to Soldiers, this consultant network standardized surgical treatment for soldiers during the war.4
“Circular letters” (official correspondence distributed widely to disseminate information) to military forward surgical units, with in-person follow-up, represented the primary means of achieving optimal “end results.” Regarding one of his first circular letters, Dr. Churchill noted, “Wound infection and suppuration emerged as one of the major considerations as it has been in every war since the dawn of history.” To wit, he promptly chastised sloppy dressing techniques and decried the practice of dousing wounds in sulfa powder rather than debriding devitalized tissue. One of his deployed colleagues, Frank Berry, MD, FACS, observed:
“Such were the initial days of Dr. Churchill and our own fledgling period, feeling our way with treatments, watching the experiences of others and finally learning under his guidance that adequate, clean surgery, carefully performed, was the primary need in war, that the sulfonamides and penicillin and antimicrobials were adjuncts but never substitutes.”4
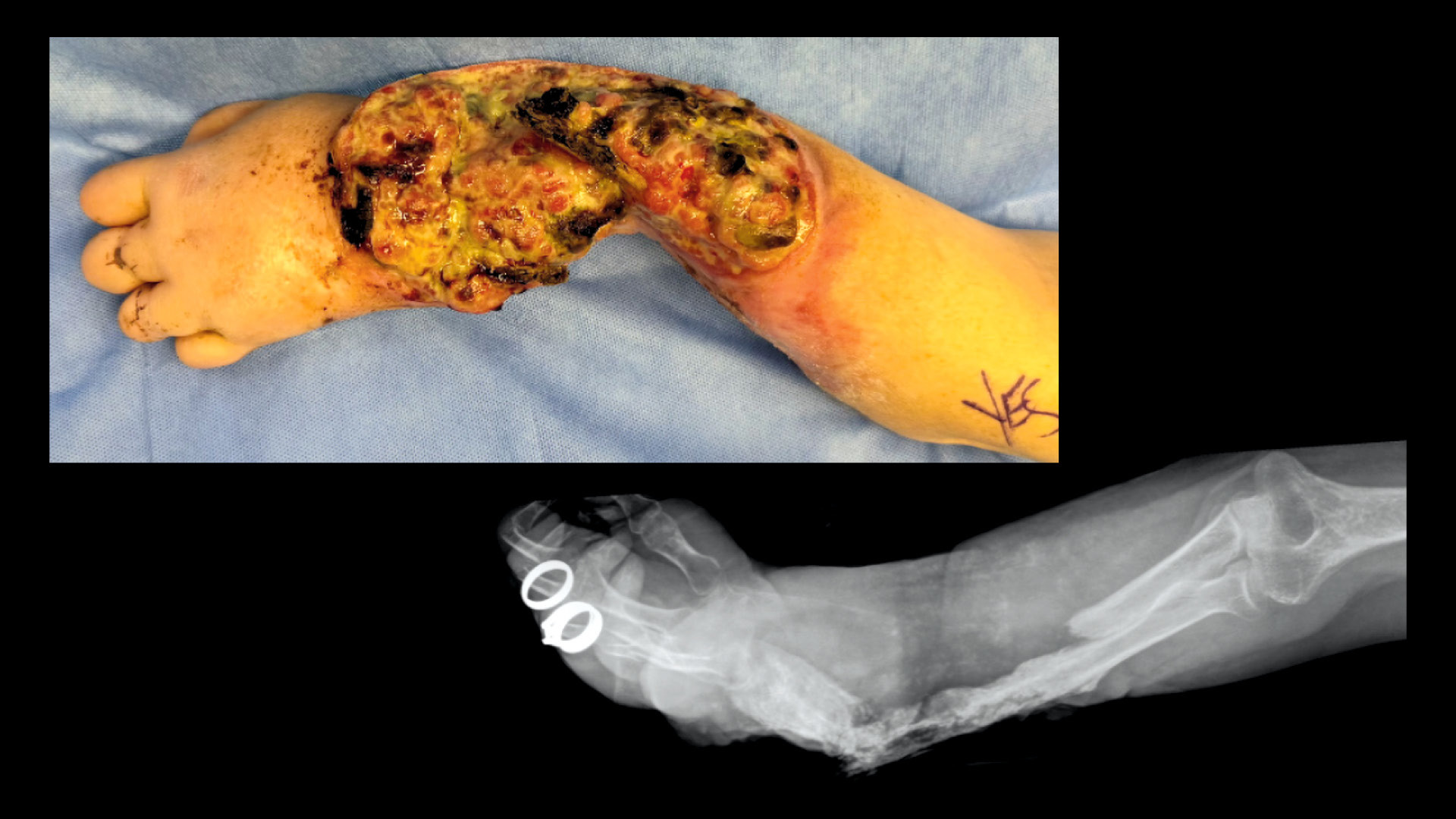
Dr. Churchill also challenged prior dogma in the management of infected hemothorax. In WWI, wide decortication, open drainage, and closure by secondary intention left patients severely disfigured. Instead, he promoted primary closure after decortication and debridement leading to superior functional results (see Figure).
“Even after the vast experience of World War II, I had to defend primary closure of an infected hemothorax at one of the first meetings of the American Association for Thoracic Surgery. Evarts Graham still could not accept this because it was a departure from a principle he had stood for in the era when streptococcus empyema was rampant.”4
Figure. Comparison of infected hemothorax outcomes from WWI (left) and WWII (right). (Credit: Army Medical Department Center of History & Heritage)
Data Collection and Academic Conferences
According to Dr. Churchill, “Opinions and impressions are plentiful and cheap, particularly under the emotional tension of a world at war. Facts are rare and precious. Complete data are next to impossible to obtain under combat conditions.”4
Nevertheless, he relentlessly pursued data collection to the extent that was possible. Established during WWI, the National Research Council laid the foundation for scientific research during WWII. Having served on the Council’s Subcommittee on Thoracic Surgery, Dr. Churchill was intimately familiar with this organization. He leveraged their scientific credibility to establish an in-theater research program on shock. Efforts to systematically record combat injuries began with the Board for the Study of the Severely Wounded in WWII and continued with the Vietnam Vascular Registry at what was then Walter Reed General Hospital. These initiatives motivated establishment of the Joint Theater Trauma Registry, now known as the Department of Defense Trauma Registry.
During the war, surgeons met intermittently to discuss their experiences and observations. By tracking outcomes and sharing best practices based on these results, surgeons not only improved clinical care but also led the dissemination of doctrine and training across hospital units. Dr. Churchill quipped, “Doctors are addicted to medical meetings where they can mingle with each other and talk shop to their hearts’ content” thus implying these events also served to boost morale during a grueling yearslong tour of duty.4
Dr. Churchill recorded the proceedings of two major conferences during his tour (see Table) in addition to multiple smaller meetings. The final conference in Rome served as an international surgical extravaganza. Held at the Eastman Dental Clinic and hosted by the Royal Army, the agenda proved expansive, but ultimately, most discussions returned to wound management.
Following this meeting, the US attendees decamped for a debriefing under Dr. Churchill’s leadership at the Excelsior Hotel, which was the Allied Headquarters in Rome, to reflect on what they had heard over the previous 5 days. Wound care, including counter-incisions, bone fragment removal, and amputation care, were reviewed. Lieutenant Colonel Michael E. DeBakey, MD, FACS, visiting from the Surgeon General’s office, remarked that diverting colostomies for rectal injuries should be brought up as separated stomas—a topic of discussion that persisted for decades afterward, ultimately landing in favor of loop stomas providing adequate diversion.
After the war, attendees at the meeting, including neurosurgeon Eldridge Campbell, MD, FACS, and orthopaedic surgeon Oscar Hampton, MD, founded the Excelsior Surgical Club with Dr. Churchill as the sole “Honor Member.”5 This group met annually for fellowship, intellectual exchange, and preservation of hard-learned lessons during combat. To support this same mission and approach in a modern context, the Excelsior Surgical Society was re-established in 2015 by the Military Health System Strategic Partnership with the American College of Surgeons (MHSSPACS).
Dr. Churchill also spoke at numerous medical and surgical society meetings in the US during his brief leave, and for years after the war. A master storyteller, he illustrated the advances made during the war for members of the Yale Medical Society in March 1946. With timely resuscitation and expert surgical intervention, a mortally wounded patient with a destructive thoracoabdominal injury survived to return home to the US 6 weeks later.
“The case of this particular soldier is admittedly dramatic, partly because the missile reached the heart. Aside from that it may be taken as representative of emergency forward surgery in World War II. In no way can it be passed by as a single lucky episode or stunt.”4
Drs. DeBakey, Churchill, and many others also disseminated their knowledge in written form. Dr. DeBakey edited several volumes of the Medical History of World War II and also advocated for founding the National Library of Medicine. In Surgeon to Soldiers, mentioned earlier in this column, Dr. Churchill offers a more intimate account of the sacrifices made by civilian surgeons during WWII.
Dr. Danielle Holt is a general surgeon and associate dean for admissions and recruitment at the Uniformed Services University School of Medicine in Bethesda, MD.
Dr. Jeremy Cannon is a trauma surgeon and professor of surgery at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia, PA.
References
Combs LC, Zwischenberger JB. Fred W Rankin, MD: A man of medicine during a time of war and change. J Am Coll Surg. 2011;212(4):e13-e23.
Moore EE, Knudson MM, Schwab CW, Trunkey DD, et al. Military-civilian collaboration in trauma care and the senior visiting surgeon program. N Engl J Med. 2007;357(26):2723-2727.
Cannon JW, Fischer JE. Edward D. Churchill as a combat consultant: Lessons for the senior visiting surgeons and today's military medical corps. Ann Surg. 2010;251(3):566-572.
Churchill ED. Edward D. Churchill’s Surgeon to Soldiers: Diary and Records of the Surgical Consultant, Allied Force Headquarters, World War II: 2024 Edition with Modern Commentary. Philadelphia: Wolters-Kluwer; 2024.
Cannon JW. Expeditionary surgeons: Essential to surgical leadership in World War II and today. J Am Coll Surg. 2024;238(5):785-793.