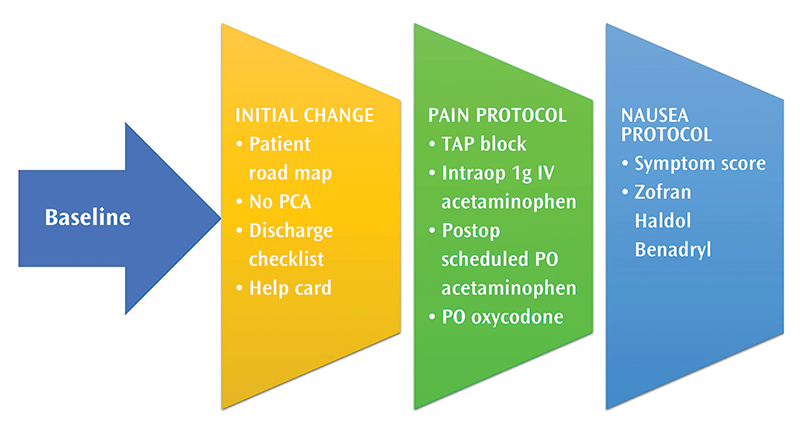
In the first stage of implementation, on the day of surgery before the operation, each patient is given a scopolamine patch. Intraoperatively, anesthesia administered 1 g intravenous (IV) acetaminophen. Our first postoperative intervention was to eliminate patient-controlled analgesia (PCA), which required the engagement of anesthesia and the pain service, as well as the floor nurses. Nursing was engaged via in-service teaching facilitated by charge nurses, as well as the surgeons.
The next step was implementation of a global reduction in postoperative narcotic use, again by reeducating the nurses on the bariatric patient unit and setting our patients’ outpatient expectations. Along with the intraoperative acetaminophen, patients are given scheduled oral (PO) acetaminophen, as needed (PRN) oxycodone, and rescue PRN morphine based on strict pain score guidelines. Patients were discharged with 10 tabs of 5 mg oxycodone.
Our second stage introduced intraoperative transversus abdominal plane (TAP) and rectus sheath blocks8-9 using 60 mL 0.25 percent Marcaine with 1 percent epinephrine expanded to 90 mL, administered by the surgeon intraoperatively via laparoscopic visualization. Our patients were discharged with only five tabs of 5 mg PO oxycodone.
In the third stage, we introduced an aggressive standardized anti-nausea protocol, which required engagement of both preoperative and postoperative nursing staff on the proper sequence and timing of ondansetron, haldol, and diphenhydramine. This step required implementing a nausea score, which would guide the administration of the antiemetic. The house staff was briefed to avoid disrupting the protocol with adjunct anti-emetics. We also implemented an inpatient checklist with hourly walking and oral intake goals. Each sequential step required physician-led education of the house officers, as well as changing electronic order sets with help from bariatric office coordinators and the university’s information technology department.
Resources used and skills needed
With respect to staffing, these interventions were primarily driven by two surgeon champions and involved the entire staff of our bariatric nursing unit, who received training from our nursing champion. Office staff within the bariatrics program—particularly our bariatric program manager, who helped implement the information technology changes, and the division’s clinical reviewer—were integral.
Minor additional costs were incurred intraoperatively to administer bupivacaine transversus abdominus plane blocks. MBSAQIP membership was a fixed cost already within the division’s budget. No additional funding was allocated to this intervention.
Results
We retrospectively analyzed data collected via MBSAQIP on patients undergoing laparoscopic Roux-en-Y gastric bypass from 2014 to 2018. These patients were broken into groups based on each stage’s implementation dates. LOS data were analyzed via t-test, and readmissions were analyzed using the Fischer exact test. Our LOS decreased significantly with implementation of the full bundle compared with baseline (1.66 days versus 1.33 days, p = 0.027). Each individual intervention was then benchmarked against the baseline and the previous intervention. When each stage was individually evaluated, introduction of TAP blocks was shown to have a significant impact on LOS, decreasing from 1.79 to 1.5 days (p = 0.04). Our 30-day readmission rate throughout the entire implementation decreased slightly, though not significantly (5.6 percent vs. 3.6 percent, p = 0.14). We were thus able to reduce LOS without increasing readmissions. Unfortunately, we were unable to capture consistent pain or nausea scores, largely because of the challenges associated with implementing a new electronic medical record.
Despite having no direct measure of pain or nausea during our interventions in this austere data environment, we knew 75 percent of readmissions were pain and/or nausea related, and thus, particularly with respect to early readmissions, the new protocol likely was effective in treating our postoperative patients’ pain and nausea. Patients were able to go home earlier and returned to the hospital at the same rate because we were better able to control their postoperative pain and nausea.
Challenges
Lacking reliable pain and nausea data within our electronic medical record system led us to implement our protocol and measure outcomes using surrogate data markers (such as LOS and readmission rates). The challenges encountered during this quality improvement project have led to improved processes to capture these specific data within our electronic medical record.
Because implementation was carried out in stages, we were able to have regular meetings with nursing as each new step was introduced. This approach meant change went more smoothly; however, it did require more frequent updates of personnel and readjustments. Furthermore, various national drug shortages forced us to use an alternative TAP block medication (liposomal bupivacaine) for several months in 2018.10
In addition, nursing staff had to be reengaged several times per year as a result of nursing staff turnover and because our mixed general surgery unit was simultaneously implementing both bariatric as well as colorectal enhanced recovery pathways.
Tips for others
Reliable data are essential when planning a quality improvement project. The use of several independent data sources will increase the chance of success. In this instance, the main outcome data (LOS and readmissions) came from the MBSAQIP registry, which is housed within the bariatric program. The more granular data (pain and nausea scores, narcotic and antiemetic use) were retrieved from the electronic health record. Use of multiple sources means that failure of one data source still leaves a usable, albeit more limited, data set.
Nursing engagement and buy-in is the key to implementing new patient care protocols. In addition, if house staff provide some aspects of patient care they must always be abreast of changes and implementations of new portions of the protocol because they are on the front lines for nursing calls and order entry. They also can be used as points of contact to educate nursing and ancillary staff.
Departmental support should follow easily if cost and LOS can be decreased. Demonstrating cost savings and reductions in LOS requires data analysis and review periodically as the intervention is implemented.
Sustaining change requires focused and unwavering pressure. At least one or two primary stakeholders and champions must be involved. Having a passionate, steady, and vocal advocate keeps these projects on track and moving forward. Interventions should be supported with data from the literature, as well as expert provider consensus.
Communication via national meetings with colleagues and with other experts can lead to new ideas. Much of our protocol was pieced together via communal experiences and communication throughout the bariatric surgery community.
References
- Hahl T, Peromaa-Haavisto P, Tarkiainen P, Knutar O, Victorzon M. Outcome of laparoscopic gastric bypass (LRYGB) with a program for enhanced recovery after surgery (ERAS). Obes Surg. 2016;26(3):505-511.
- Singh PM, Panwar R, Borle A, et al. Efficiency and safety effects of applying ERAS protocols to bariatric surgery: A systematic review with meta-analysis and trial sequential analysis of evidence. Obes Surg. 2017;27(2):489-501.
- Lassen K, Soop M, Nygren J, et al. Consensus review of optimal perioperative care in colorectal surgery: Enhanced Recovery After Surgery (ERAS) Group recommendations. Arch Surg. 2009;144(10):961-969.
- Voellinger DC, Morton V, Kolasch C, Carraro EA, Duggins CJ, Benonis JG. Implementation of a bariatric ERAS program at a community hospital improves both perioperative and 30-day outcomes and reduces cost. Surg Obes Relat Dis. 2018;14(11):S21-S22.
- King AB, Spann MD, Jablonski P, et al. An enhanced recovery program for bariatric surgical patients significantly reduces perioperative opioid consumption and postoperative nausea. Surg Obes Relat Dis. 2018;14(6):849-856.
- Thorell A, MacCormick AD, Awad S, et al. Guidelines for perioperative care in bariatric surgery: Enhanced recovery after surgery (ERAS) society recommendations. World J Surg. 2016;40(9):2065-2083.
- Mannaerts GH, Van Mil SR, Stepaniak PS, et al. Results of implementing an enhanced recovery after bariatric surgery (ERABS) protocol. Obes Surg. 2016;26(2):303-312.
- Sinha A, Jayaraman L, Punhani D. Efficacy of ultrasound-guided transversus abdominis plane block after laparoscopic bariatric surgery: A double blind, randomized, controlled study. Obes Surg. 2013;23(4):548-553.
- Albrecht E, Kirkham KR, Endersby RV, et al. Ultrasound-guided transversus abdominis plane (TAP) block for laparoscopic gastric-bypass surgery: A prospective randomized controlled double-blinded trial. Obes Surg. 2013;23(8):1309-1314.
- Ziemann-Gimmel P, Marema R, Goldfarb A, Connelly M. Does local wound infiltration with liposomal bupivacaine (Exparel) reduce narcotic requirements or length-of-stay after bariatric operations? Surg Obes Relat Dis. 2016;12(7):S124-S125.