With traditional perioperative care, day-of-surgery cancellations and surgical complications can result from multiple factors, including poor blood sugar control, inadequately managed disease processes, frailty, poor nutrition, smoking, delirium, and unaddressed medications.
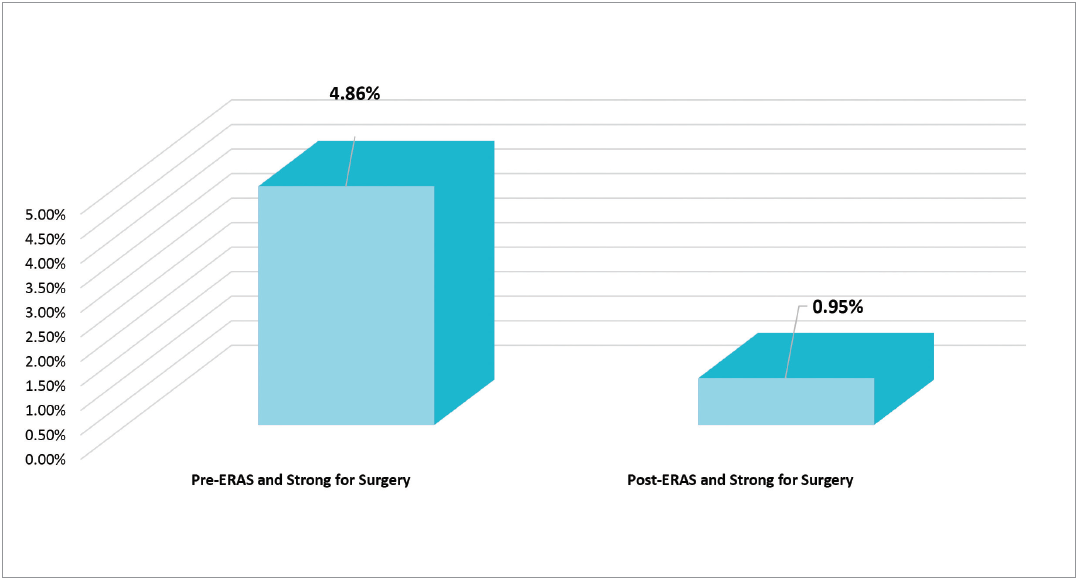
In 2016, American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP®) data for colorectal surgery at CHRISTUS St. Michael Health System (CSMHS), Texarkana, TX, demonstrated an overall postoperative occurrence rate of 32.7 percent, an average length of stay (LOS) of 7.4 days, and average variable costs of $6,346, including labs, radiology, pharmacy, and supplies. In the ambulatory care unit, blood sugar control (blood glucose <200 mg/dl) on the day of surgery was 87.7 percent, and the day-of-surgery cancellation rate was 4.9 percent.
CSMHS is a faith-based, community, not-for-profit, 354-bed acute care facility that provides health care services in 13 predominately rural counties in northeast Texas, southeast Oklahoma, and southwest Arkansas. To improve patient outcomes, CSMHS initiated a nurse practitioner (NP)-driven, hospital-based preoperative clinic. The clinic was developed using the principles of Enhanced Recovery After Surgery/(ERAS) Strong for Surgery checklists and guidelines. In the preoperative clinic, the NP captures ACS NSQIP variables, identifies patient risk factors using Strong for Surgery checklists, and follows ERAS guidelines to prepare patients for surgery. The goal is to enhance the surgical care of the patient, reduce the LOS without increasing readmissions, minimize postoperative complications, decrease health care costs, and increase patient quality of life and satisfaction.
Putting the plan in place
In 2016, the CSMHS quality department team attended the annual ACS Quality & Safety Conference, and through the conference sessions gained a better understanding of ERAS principles and Strong for Surgery guidelines. We brought these concepts back to our institution and began to implement these two programs in the hospital.
The team gathered information on successful ERAS programs across the nation, and in 2016 our medical executive committee approved a colorectal ERAS program as a process improvement project for our hospital. It became apparent that a preoperative clinic within the hospital would serve as a gateway for the ERAS program and would help to ensure the principles were properly implemented. Once the original Strong for Surgery guidelines were published, they were added to the program, and the preoperative clinic was on its way to implementation.
The ERAS principles were introduced at the team’s initial meeting in September 2016. Shortly after this meeting, we began to develop the ERAS algorithms and measurements. We completed the preoperative, intraoperative, and postoperative algorithms in February 2017.
The team hired a preoperative clinic NP in early 2017, and by April 2017 we began piloting ERAS on colorectal surgery patients. We also introduced the nutrition, blood sugar, medication, and smoking Strong for Surgery checklists to the team and finalized our program logo and education booklet. During this time, our surgeon champion began providing education on ERAS and Strong for Surgery guidelines to the community surgeons and hospital staff.
The clinic officially became operational in June 2017, with ERAS colorectal and the first four checklists for Strong for Surgery. We began to track the ACS NSQIP/ERAS variables for colorectal surgery. When the ACS introduced the Strong for Surgery checklists for delirium, prehabilitation, safe and effective pain control, and patient directives, we added them to our repertoire.
Early in 2018, the team began planning for ERAS orthopaedic operations and the integration of ERAS with the Agency for Healthcare Research and Quality Safety Program for Improving Surgical Care and Recovery (ISCR). In October 2018, we implemented orthopaedic ERAS and ISCR for knee replacement, hip replacement, and hip fractures. The team now is implementing the ERAS and ISCR gynecology guidelines.
In preparation for implementation, the surgeon champion provided education to the community surgeons and select hospital staff. The clinical education department provided house-wide education, and all nursing associates were required to complete online education modules on care provided to the ERAS patient. The team also developed and implemented our data collection methods.
We created ERAS education booklets for patients and their family members. These pamphlets were distributed to physician offices where education is initiated. Brochures also are provided in the preoperative clinic. The NP was responsible for educating patients on preoperative, postoperative, and discharge instructions, as well as applying the Strong for Surgery checklists to each patient.
The surgeon and anesthesiologist write the pre- and postoperative ERAS orders, and nursing staff is responsible for carrying them out.
We assembled a multidisciplinary team from the following areas of the hospital:
- Administration
- Anesthesia
- Case management
- Clinical information
- Critical care
- Dietary
- Marketing
- Nurse education
- Pharmacy
- Physician office personnel
- Physical therapy
- Postoperative nursing
- Quality outcomes
- Respiratory
- Risk management
- Surgeon champion
- Surgical services
No additional costs or funding beyond normal hospital operations were necessary to implement and maintain the quality improvement (QI) program.
Results
We obtained data using the ACS NSQIP database. Additional information was obtained during the preoperative visit, hospital stay, and postoperative phone calls, which were conducted two months after the surgical procedure.
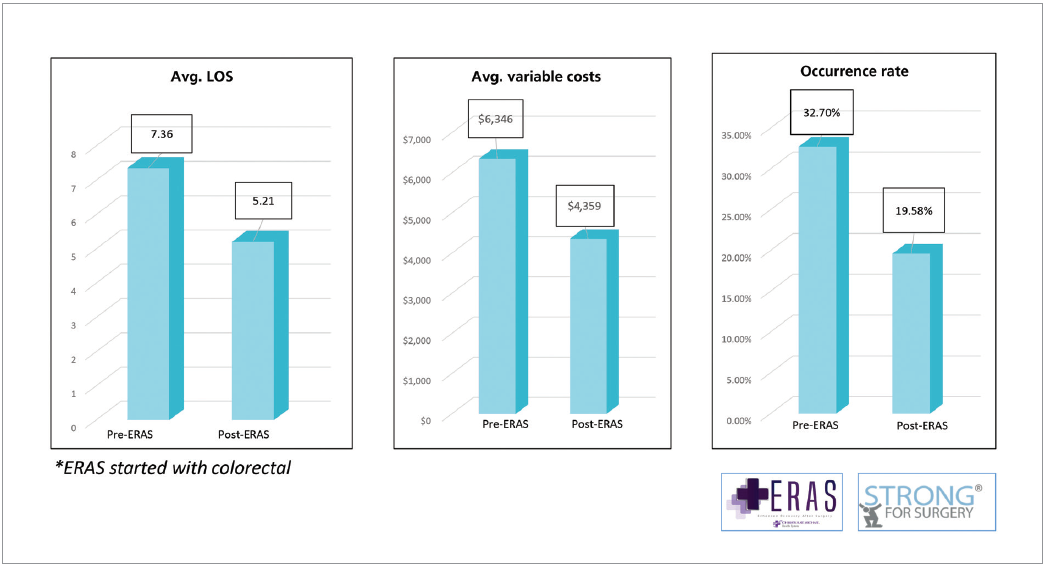
Analysis of colorectal ERAS data for one year indicated that patient LOS decreased from 7.3 days to 5.2 days (see Figure 1). The average variable costs were reduced from $6,346 to $4,359. Postoperative occurrences as defined by ACS NSQIP decreased from 32.7 percent to 19.6 percent.
Figure 1. Year one ERAS—colorectal results