Abstract
Background
A 27-year-old woman with a history of Marfan syndrome presented to the trauma bay in acute respiratory distress following a motor vehicle collision where she was a pedestrian. She sustained bilateral femur fractures, and initial imaging uniquely identified fat emboli in transit within the bilateral femoral veins, with subsequent progression to fulminant fat embolism syndrome (FES).
Summary
We present a case of FES developing in the context of traumatic bilateral femoral fractures. The patient initially presented with significant respiratory distress and a Glasgow Coma Scale score of 14; cross-sectional imaging at that time remarkably demonstrated fat emboli in transit within both femoral veins. Shortly after admission, she experienced an acute neurological deterioration with right-sided hemiparesis, consistent with a cerebrovascular accident secondary to paradoxical embolization through a previously undiagnosed patent foramen ovale. Following bilateral femoral intramedullary nailing, her neurological status gradually improved. She was discharged to an acute rehabilitation facility on post-trauma day thirteen and required an extended rehabilitation course to regain her pre-trauma functional baseline.
Conclusion
Fat embolism syndrome is often discussed as a dreaded complication of traumatic injury yet relatively uncommon in clinical practice. The direct visualization of peripheral fat emboli in transit on cross-sectional imaging, as occurred in this case, is exceptionally rare. This report underscores that even in the absence of such distinct radiographic findings, clinicians must maintain a high index of suspicion for FES in at-risk patients to ensure the timely institution of aggressive supportive care and prompt surgical stabilization of fractures, which is critical to mitigate further embolic burden.
Key Words
fat embolus syndrome; trauma surgery; long bone fracture
Case Description
A 27-year-old woman with a known history of Marfan syndrome sustained polytrauma as a pedestrian struck by a motor vehicle and was transported by Emergency Medical Services to the trauma bay. Her primary survey revealed an intact airway and spontaneous respirations; however, she exhibited significant hypoxemia, necessitating supplemental oxygen via a non-rebreather mask at 15 L/min to maintain oxygen saturations above 92%. Her initial Glasgow Coma Scale (GCS) score was 14 (Eye Opening 4, Verbal Response 4, Motor Response 6). Examination demonstrated obvious bilateral thigh deformities, characterized by foreshortening and external rotation of both lower limbs, though distal motor function and sensation were preserved.
The secondary survey was notable for abrasions to the forehead and anterior chest, in addition to a fractured left fifth digit. A chest radiograph was unremarkable. Radiographs of the lower extremities confirmed bilateral displaced femoral shaft fractures (Figure 1). Bilateral Hare traction was applied, and the patient proceeded to a trauma pan-computed tomography (CT) scan. CT imaging of the head, cervical spine, and chest showed no acute traumatic abnormalities. However, the CT scan of the abdomen and pelvis incidentally revealed real-time fat emboli (density approximately -100 Hounsfield units) in transit within the bilateral femoral veins (Figure 2); this study was otherwise negative for acute intra-abdominal or pelvic trauma.
Figure 1. Bilateral Displaced Femoral Shaft Fractures at Presentation. Published with Permission
Venous thromboembolism (VTE) prophylaxis with enoxaparin was initiated. Due to persistent hypoxemia, she was transferred to the Trauma Surgical Intensive Care Unit (TSICU) for ongoing oxygen therapy, continuous respiratory monitoring, and frequent neurovascular assessments while awaiting operative fixation of her femoral fractures. Throughout this initial period, she did not require positive pressure ventilation or endotracheal intubation.
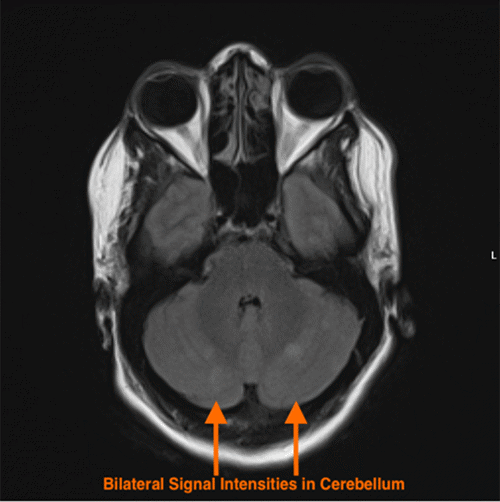
Approximately six hours after admission to the TSICU, the patient experienced an acute neurological deterioration, manifesting as right upper extremity (RUE) weakness and dysarthria. Urgent magnetic resonance imaging (MRI) of the brain was performed, which demonstrated diffuse small vessel ischemic infarcts affecting bilateral cerebellar hemispheres (Figure 3), presumed to be secondary to paradoxical fat embolization. This diagnosis was further supported by an emergent transthoracic echocardiogram, obtained immediately following the MRI, which identified a Grade 1 patent foramen ovale (PFO) (Figure 4). In light of these findings and to mitigate further propagation of fat emboli from the unstable femur fractures, the patient was taken emergently to the operating room by the Orthopaedic Surgery service for bilateral femoral external fixation, serving as a damage control measure until she achieved greater neurological stability.
Figure 3. MRI of Cerebellar Embolic Infarcts. Published with Permission
Following external fixation, the patient's RUE motor strength gradually improved, although mild dysarthria persisted. On post-trauma day seven, she underwent definitive, uncomplicated bilateral femoral intramedullary nailing. Postoperatively, her dysarthria resolved rapidly; however, she initially remained dependent for all activities of daily living (ADLs), including transfers, toileting, showering, and dressing. On post-trauma day 13, she was discharged to an acute inpatient rehabilitation facility.
The patient made excellent progress during her 26-day stay in acute rehabilitation, engaging in intensive physical and occupational therapy, and ultimately achieved independence in her ADLs prior to discharge. By post-trauma day 60, she was ambulating independently without the use of assistive devices.
Discussion
Fat embolism (FE) refers to the common phenomenon of fat globules entering the peripheral or pulmonary circulation, frequently precipitated by orthopedic procedures or significant trauma. While the mere presence of fat emboli is often subclinical and may be identified in as many as 68-82% of blunt trauma patients at autopsy, FES constitutes a distinct, life-threatening clinical entity characterized by a constellation of symptoms, classically including respiratory distress, neurological manifestations, and, less commonly, a petechial rash.1 FES, with an incidence of approximately 0.26% following pelvic and long bone fractures, is thought to arise not merely from vascular occlusion by fat globules but also from a compounded systemic inflammatory response to both the embolized fat and the initial trauma. The management of suspected FES is predominantly supportive.2-6
The prevailing pathophysiological model of FES suggests that trauma to long bones disrupts intramedullary venous sinusoids and elevates intramedullary pressure, thereby facilitating the entry of fat droplets into the venous circulation. In individuals without an intracardiac (e.g., patent foramen ovale - PFO) or significant intrapulmonary shunt, these fat droplets primarily lodge in the pulmonary microvasculature, potentially leading to acute respiratory failure. However, in the presence of such anatomical communications allowing right-to-left shunting, fat droplets can paradoxically enter the systemic arterial circulation, resulting in end-organ injury. Systemic manifestations may include renal dysfunction (oliguria, nephropathy), dermal petechiae, cerebral injury (encephalopathy, stroke-like symptoms), and ocular findings (retinal or conjunctival hemorrhages). Additionally, cytopenias have been reported, suggesting a potential impact on bone marrow function or a systemic consumptive process.6
Several diagnostic criteria have been proposed to aid in the clinical identification of FES. Gurd and Wilson’s criteria combine major findings (respiratory insufficiency, cerebral involvement, petechial rash) with various minor systemic clinical signs and laboratory abnormalities. The Lindeque guidelines place a greater emphasis on objective measures such as arterial blood gas values and the work of breathing. The Schonfeld criteria integrate clinical findings, including petechiae, with blood gas analysis and hemodynamic parameters.6
The radiographic identification of fat emboli in transit on cross-sectional imaging is an exceptionally rare occurrence, even less common than FES itself. One report described fat emboli in transit following a traumatic unilateral tibial and fibular fracture, which did not result in cardiorespiratory compromise.7 In contrast, another case report detailed a scenario similar to ours, involving a high-speed motor vehicle crash leading to a unilateral displaced femoral fracture. That patient presented with a GCS of 13, and chest imaging revealed a large, multilobulated filling defect in the right atrium. Subsequent echocardiography confirmed a PFO and characterized the atrial mass as mobile and concerning for a fat embolus in transit. Given its size and mobility, the patient underwent median sternotomy for atrial mass excision and PFO closure, with final pathology confirming bone marrow origin.8 While a PFO provides a clear conduit for paradoxical embolism, neurological symptoms in FES have also been documented in patients without a detectable PFO, suggesting that fat microemboli may also traverse intrapulmonary arteriovenous shunts.9
Our case of visualized fat emboli in transit is notable for its bilateral nature in the femoral veins and the patient's rapid deterioration into significant respiratory and neurologic compromise. Equally noteworthy was the prompt improvement observed following external fixation of the femur fractures, theoretically attributable to the stabilization of fracture sites and consequent reduction in the ongoing propagation of the embolic burden. External fixation is often employed as a damage control orthopedic strategy, particularly in polytrauma patients, to stabilize the medullary canal during the initial resuscitation period, as definitive intramedullary nailing (IMN) carries a risk of inducing further embolization. Beyond prompt fracture fixation and comprehensive supportive care (including maintenance of oxygenation and ventilation), specific targeted therapies for FES, such as heparin, hypertonic glucose, and aspirin, were considered but have not demonstrated conclusive clinical benefit.4,5 Prophylactic corticosteroids have been investigated for the prevention of FES, with some systematic reviews and meta-analyses suggesting a potential reduction in FES incidence. However, these studies are often constrained by small sample sizes, heterogeneous dosing regimens, and varied treatment durations, which collectively limit the quality of evidence.10,11 Corticosteroids were not administered to our patient, as FES was already established upon her presentation. Therefore, our management strategy centered on prompt surgical stabilization of her bilateral fractures, aggressive supportive care in a monitored setting, and subsequently, intensive rehabilitation to facilitate her return to baseline functional status.
Conclusion
Clinicians must maintain a high index of suspicion for FES in patients sustaining traumatic long bone fractures, as this potentially severe complication necessitates prompt interdisciplinary management and aggressive supportive care. While the incidental radiographic identification of fat emboli in transit, particularly when correlated with classic symptoms, can support the clinical diagnosis, such findings are unlikely to fundamentally alter the primary management strategy—which remains centered on supportive care—barring exceptionally dramatic presentations, such as a large, mobile intracardiac fat embolus posing an immediate threat of massive paradoxical embolism. Recovery from the significant neurological sequelae that can accompany FES with cerebral embolization often requires intensive and prolonged rehabilitation services to facilitate a return toward baseline functional status.
Lessons Learned
Fat embolism syndrome with directly visualized fat emboli in transit represents an uncommon clinical entity, and a definitive, evidence-based management paradigm for this specific scenario remains incompletely elucidated. The favorable progression of our patient with comprehensive supportive care and prompt femoral fracture stabilization underscores the critical importance of early orthopedic intervention aimed at limiting further embolic propagation from unstable fracture sites. Furthermore, this case reinforces the necessity of a well-coordinated, interdisciplinary approach to optimize outcomes for traumatically injured patients at risk for, or actively manifesting, FES.
Authors
Roberson JL; Kim P
Author Affiliations
Department of Surgery, Hospital of the University of Pennsylvania, Philadelphia, PA 19104
Corresponding Author
Jeffrey L. Roberson, MD, MBA
Hospital of the University of Pennsylvania
3400 Spruce Street
Maloney 4
Philadelphia, PA 19104
Email: jeffrey.roberson@pennmedicine.upenn.edu
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding/Support
The authors have no relevant financial relationships or in-kind support to disclose.
Received: July 10, 2024
Revision received: October 20, 2024
Accepted: December 3, 2024
References
- Rothberg DL, Makarewich CA. Fat embolism and fat embolism syndrome. J Am Acad Orthop Surg. 2019;27(8):e346-e355. doi:10.5435/JAAOS-D-17-00571
- Eriksson EA, Pellegrini DC, Vanderkolk WE, et al. Incidence of pulmonary fat embolism at autopsy: an undiagnosed epidemic. J Trauma. 2011;71(2):312-315. doi:10.1097/TA.0b013e3182235778
- Mudd KL, Hunt A, Matherly RC, et al. Analysis of pulmonary fat embolism in blunt force fatalities. J Trauma. 2000;48(4):711-715. doi:10.1097/00005373-200004000-00019
- Tzioupis CC, Giannoudis PV. Fat embolism syndrome: what have we learned over the years? Trauma (Lond). 2011;13(4):259-281. doi:10.1177/146040861101300403
- Mellor A, Soni N. Fat embolism. Anaesthesia. 2001;56(2):145-154. doi:10.1046/j.1365-2044.2001.01724.x
- Kwon J, Coimbra R. Fat embolism syndrome after trauma: what you need to know. J Trauma Acute Care Surg. 2024;97(4):505-513. doi:10.1097/TA.0000000000004434
- Chowdhary V, Metha V, Bajaj T, Scheiner J. Rare imaging of a known entity: fat embolism seen on CT in lower extremity vein after trauma. Radiol Case Rep. 2017;12(3):488-490. doi:10.1016/j.radcr.2017.03.014
- Larson EE, Moe DM, Craig JC, Hoffman JRH. Fat embolism in transit: report of a rare phenomenon. JTCVS Tech. 2021;9:97-99. doi:10.1016/j.xjtc.2021.05.018
- Husebye EE, Lyberg T, Røise O. Bone marrow fat in the circulation: clinical entities and pathophysiological mechanisms [published correction appears in Injury. 2007 Oct;38(10):1224]. Injury. 2006;37(suppl 4):S8-S18. doi:10.1016/j.injury.2006.08.037
- Bederman SS, Bhandari M, McKee MD, Schemitsch EH. Do corticosteroids reduce the risk of fat embolism syndrome in patients with long-bone fracture? A meta-analysis. Can J Surg. 2009;52(5):386-393. PMID:19865539.
- Sen RK, Tripathy SK, Krishnan V. Role of corticosteroid as a prophylactic measure in fat embolism syndrome: a literature review. Musculoskelet Surg. 2012;96(1):1-8. doi:10.1007/s12306-011-0155-7