Abstract
Background
Primary pulmonary sarcomas are rare neoplasms, constituting only a small percentage of lung cancers. They typically present with common pulmonary symptoms, such as cough or shortness of breath, and are usually identified as solid masses on preoperative imaging. Lobectomy with negative margins represents the preferred surgical approach.
Summary
This report describes a case of a 68-year-old female who presented with a large, heterogeneous pleural effusion, with septations suggestive of loculation, and no evidence of pulmonary masses on imaging. Following pleural fluid sampling via thoracentesis, the patient underwent pleural drainage and decortication. Upon entry into the pleural space, a large cystic mass occupying the entire lower lobe of the lung was noted. A left lower lobectomy with mediastinal lymph node dissection was performed. Final pathological examination revealed that lymph nodes from multiple mediastinal stations were benign. Final examination of the lung specimen revealed an estrogen and progesterone receptor-positive mesenchymal tumor with heterologous chondromatous elements, consistent with a primary pulmonary sarcoma.
Conclusion
While adequate preoperative evaluation and surgical planning is ideal in oncologic surgery, this case illustrates the importance of adaptability when encountering an unexpected pathology.
Key Words
sarcoma; VATS; thoracotomy; lobectomy
Case Description
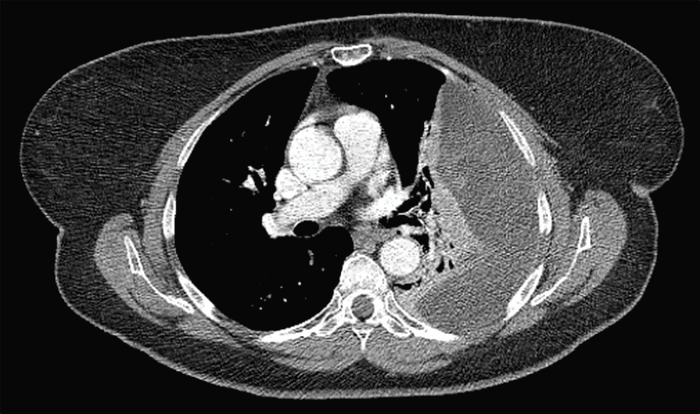
A 68-year-old female presented to our institution with abdominal pain, shortness of breath, and right-sided chest pain. A chest radiograph, obtained as part of a routine wellness visit, incidentally revealed a left-sided pleural effusion and ipsilateral atelectasis (Figure 1). At that time, the patient was asymptomatic, without shortness of breath, chest pain, cough, fever, or weight loss. A CT scan of the chest demonstrated a large, heterogeneous pleural effusion with internal septations, suggestive of loculation, and no evidence of masses or nodules within the lung parenchyma (Figure 2). The patient subsequently underwent ultrasound-guided thoracentesis, yielding only 30 mL of pleural fluid, which was sent for cytology, cell counts, cultures, and chemistry analysis. Pleural fluid analysis returned negative for malignancy, with benign mesothelial cells and chronic inflammatory cells.
Figure 1. Preoperative Chest Radiograph. Published with Permission
Figure 2. Preoperative Computed Tomography of the Chest. Published with Permission
Following thoracentesis, the cardiothoracic surgery team was consulted to consider further surgical intervention for drainage and decortication of the complex, loculated pleural effusion. The patient’s past medical history included hypertension, hyperlipidemia, and type 2 diabetes mellitus. She denied any history of smoking, but she did report occupational asbestos exposure as a factory worker. As thoracentesis failed to achieve adequate drainage of the effusion, the surgical team elected to proceed with a left-sided video-assisted thoracoscopic surgery (VATS) for drainage and decortication of the left pleural space.
A posterolateral thoracotomy incision was made. The inferior pulmonary ligament was divided, and hilar and subcarinal lymph nodes were dissected and sent for pathology. The left lower lobe bronchus was identified, isolated, and clamped to ensure upper lobe expansion, and subsequently transected with a stapler. Next, branches of the pulmonary artery and vein were dissected and ligated with a stapler. The fissure was incompletely developed, requiring an additional thick tissue staple fire to separate the upper and lower lobes. The mass was then able to be removed from the chest (Figure 3). Lymph nodes at the aortopulmonary window region were identified and dissected for pathology. Two chest tubes were placed, and the patient was transferred to the ICU for further monitoring.
Figure 3. Gross Pathology of Resected Pulmonary Sarcoma. Published with Permission
The patient’s postoperative course was uncomplicated, and she was discharged on postoperative day seven. A postoperative chest radiograph, obtained two weeks after surgery, demonstrated good expansion of the upper lobe with a small residual effusion (Figure 4).
Figure 4. Postoperative Chest Radiograph. Published with Permission
Pathological examination revealed benign lymph nodes from stations 5, 7, 8, and 10. Final examination of the lung specimen revealed an estrogen and progesterone receptor-positive mesenchymal tumor with chondromatous heterologous elements. Further pathological examination demonstrated predominant stromal structures, lined by an epithelioid component. Immunostains showed spindle cells positive for progesterone receptors, estrogen receptors, desmin, caldesmon, SMA, CD10, and vimentin. The final pathology report indicated that, based on these histological features and the immunohistochemical profile, this tumor was a very rare malignant neoplasm, likely a sarcoma or, less likely, a biphasic epithelial and stromal tumor. Based on size and grade, this tumor was classified as stage IIIB, with negative lymph nodes and negative margins. The patient in this report has continued to do well postoperatively and has followed up with oncology and radiation oncology. No further treatment with chemotherapy, radiation, or hormonal therapy was recommended, given the low suspicion for residual disease after adequate resection and the absence of parietal pleura involvement.
Discussion
Primary pulmonary sarcomas are rare, comprising less than 1% of all lung cancers.1 Patients typically present with a solid mass on imaging, necessitating careful surgical planning prior to oncologic resection.2 They most commonly affect women in the sixth and seventh decades of life, often with a history of smoking.3 Sarcomas arise from mesenchymal cells of connective tissue origin and represent a heterogeneous group of cancers, further differentiated by gross and histopathological examination.4,5 Common subtypes include synovial sarcoma, leiomyosarcoma, and, more frequently, undifferentiated sarcomas.6
Patients often present with nonspecific symptoms, and chest radiographs are frequently the initial diagnostic test. In one study of 18 patients with primary pulmonary sarcomas, 50% were asymptomatic, with the tumors discovered incidentally on routine chest radiographs.5 Preoperative evaluation typically includes CT, sputum cytology, and fiberoptic bronchoscopy. In the aforementioned study, all patients had a solid mass on preoperative CT scans, further emphasizing the atypical presentation of the current case.
Once a diagnosis is established or a high suspicion for lung cancer exists, assessment of resectability is crucial, as factors such as distant metastatic spread, invasion into local structures, and bulky nodal disease can significantly alter surgical planning.2 In the previously mentioned study of 18 patients undergoing resection of pulmonary sarcoma, only two were deemed unresectable at the time of diagnosis and underwent neoadjuvant chemotherapy. Lobectomy with negative margins is the preferred surgical approach, with large tumor size, high-grade histology, and unresectable disease conferring a worse prognosis. A large study of 365 patients with pulmonary sarcomas underscored the importance of mediastinal nodal evaluation to rule out locoregional metastasis, given the poor prognosis and high risk of recurrence in these patients.6 Adjuvant therapy is generally offered for patients with unresectable tumors or those with close margins and positive nodes.3 Multiple studies have reported 5-year survival rates for stage I tumors of approximately 50% for pulmonary sarcoma patients.7 This percentage decreases with increasing tumor stage, with 5-year survival rates estimated to be 39% for stage II and 23% for stage III.3
Conclusion
While adequate preoperative evaluation and surgical planning is ideal in the approach to oncologic surgery, our case illustrates the importance of adaptability when encountering an unexpected pathology. The surgical team successfully modified the planned approach, considering the challenges of informed consent and the need for adequate oncologic resection. This case highlights the critical role of intraoperative decision-making and the ability to deviate from the planned strategy when presented with unforeseen findings.
Lessons Learned
This case demonstrates an operative approach to an unusual and unexpected pathology. In the management of pleural effusions, initial drainage is often achieved with chest tube placement. In retrospect, had a chest tube been placed in our patient and adequate drainage not been achieved, a repeat CT scan might have revealed evidence of a mass prior to operative intervention. If a mass had been visualized, the patient might have undergone percutaneous or bronchoscopic biopsy, followed by staging PET-CT. Nevertheless, given the information available at the time of intervention, an appropriate treatment was achieved, and the patient had a favorable outcome. Surgeons must remain adaptable and prepared to modify their approach in response to changing situations encountered in the operating room.
Authors
Eckholdt Ca; Heap Jr. Db; Samra Nc; Rao VRa
Author Affiliations
- Department of Surgery, Ochsner LSU Health Shreveport Academic Medical Center, Division of Cardiothoracic Surgery, Shreveport, LA 71130
- LSU Health Shreveport School of Medicine, Shreveport, LA 71130
- Department of Surgery, Ochsner LSU Health Shreveport Academic Medical Center, Division of Trauma & Surgical Critical Care, Shreveport, LA 71130
Corresponding Author
Vyas R. Rao, MD
Department of Surgery
Ochsner LSU Health Shreveport Academic Medical Center
1501 Kings Highway
Shreveport, LA 71103
Email: vyas.rao@lsuhs.edu
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding/Support
The authors have no relevant financial relationships or in-kind support to disclose.
Received: September 28, 2023
Revision received: January 10, 2024
Accepted: February 28, 2024
References
- Gołota J, Osowiecka K, Orłowski T. Primary pulmonary sarcoma - treatment outcomes depending on the different types of radical operation. Kardiochir Torakochirurgia Pol. 2019;16(1):1-6. doi:10.5114/kitp.2019.83938.
- Quint LE. Lung cancer: assessing resectability. Cancer Imaging. 2003;4(1):15-18. Published 2003 Oct 1. doi:10.1102/1470-7330.2003.0028.
- Robinson LA, Babacan NA, Tanvetyanon T, Henderson-Jackson E, Bui MM, Druta M. Results of treating primary pulmonary sarcomas and pulmonary carcinosarcomas. J Thorac Cardiovasc Surg. 2021;162(1):274-284. doi: 10.1016/j.jtcvs.2020.03.179.
- Hashimoto H, Tsugeno Y, Sugita K, Inamura K. Mesenchymal tumors of the lung: diagnostic pathology, molecular pathogenesis, and identified biomarkers. J Thorac Dis. 2019;11(Suppl 1):S9-S24. doi:10.21037/jtd.2018.12.04.
- Travis WD, Brambilla E, Nicholson AG, et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J Thorac Oncol. 2015;10(9):1243-1260. doi:10.1097/JTO.0000000000000630.
- Keel SB, Bacha E, Mark EJ, Nielsen GP, Rosenberg AE. Primary pulmonary sarcoma: a clinicopathologic study of 26 cases. Mod Pathol. 1999 Dec;12(12):1124-31.
- Porte HL, Metois DG, Leroy X, Conti M, Gosselin B, Wurtz A. Surgical treatment of primary sarcoma of the lung. Eur J Cardiothorac Surg. 2000;18(2):136-142. doi:10.1016/s1010-7940(00)00465-6.
- Spraker MB, Bair E, Bair R, Connell PP, Mahmood U, Koshy M. An analysis of patient characteristics and clinical outcomes in primary pulmonary sarcoma. J Thorac Oncol. 2013;8(2):147-151. doi:10.1097/JTO.0b013e318277401f.
- Petrov DB, Vlassov VI, Kalaydjiev GT, et al. Primary pulmonary sarcomas and carcinosarcomas--postoperative results and comparative survival analysis. Eur J Cardiothorac Surg. 2003;23(4):461-466. doi:10.1016/s1010-7940(03)00024-1.