Become a member and receive career-enhancing benefits
Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
Become a member and receive career-enhancing benefits
Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
Technical Considerations for Robotic Cholecystectomy in Situs Inversus Totalis
June 23, 2025
15 MinPrintShare
Bookmark
Abstract
Background
Situs inversus totalis (SIT) is a rare, autosomal recessive condition characterized by right-sided heart, stomach, and aorta and left-sided liver, gallbladder, and inferior vena cava. Approximately 120 cases of cholecystectomy in patients with SIT have been reported; however, to our knowledge, only three reports of robotic cholecystectomy in this setting have been published. Further understanding of the technical nuances of robotic cholecystectomy in SIT can inform surgeons and promote safe surgical practice.
Summary
We present the case of a 54-year-old female with SIT who presented with acute gallstone pancreatitis. She underwent an uncomplicated multi-port, robotic-assisted cholecystectomy utilizing indocyanine green (ICG) with near-infrared fluorescence (NIF) imaging for enhanced biliary ductal identification.
Conclusion
Patients with SIT presenting with gallbladder pathology pose both diagnostic and technical challenges due to their altered anatomy. The robotic-assisted approach to cholecystectomy in SIT offers potential advantages, including the ability to perform “open-like” surgery in a minimally invasive fashion and the use of ICG with NIF imaging to facilitate intraoperative understanding of the biliary anatomy.
Key Words
situs inversus totalis; robotic cholecystectomy; surgical technique
Case Description
Since the first description of cholecystectomy in situs inversus totalis (SIT) by Campos,¹ approximately 120 cases of laparoscopic cholecystectomy in patients with SIT have been reported.² SIT, an autosomal recessive disorder, is characterized by a right-sided heart, stomach, and aorta, and a left-sided liver, gallbladder, and inferior vena cava. Laparoscopic cholecystectomy is the preferred approach in these patients.³ To our knowledge, only three prior reports of robotic cholecystectomy in SIT patients exist. This report details the clinical presentation, imaging, and technical aspects of a robotic-assisted cholecystectomy in a patient with SIT presenting to a community hospital.
A 54-year-old white woman with SIT, hypertension, gastroesophageal reflux, and a history of transabdominal hysterectomy presented to the emergency department with seven days of left upper quadrant and epigastric pain after fatty meals. Physical examination revealed left upper quadrant tenderness and a lower midline laparotomy scar. Laboratory studies showed elevated lipase (404), leukocytosis (WBC 11), and normal liver function tests. Ultrasound confirmed cholelithiasis without acute cholecystitis and demonstrated SIT anatomy. CT of the chest, abdomen, and pelvis revealed SIT, pancreatitis, and duodenitis (Figure 1A-C). MRCP, obtained per gastroenterology recommendation, was negative for choledocholithiasis (Figure 1D), and an EGD was normal. A diagnosis of gallstone pancreatitis was made.
Figure 1. Preoperative Imaging Findings. Published with Permission
(A) Dextrocardia. (B) Liver and gallbladder (white arrow) located in the left upper quadrant. (C) Acute pancreatitis (white arrow). (D) Magnetic resonance cholangiopancreatography demonstrating no choledocholithiasis (white arrow)
After extensive discussion with the patient and the gastroenterology team, robotic multiport cholecystectomy using the da Vinci Xi platform (Intuitive, CA) was planned. The Xi platform was chosen for its superior optics and indocyanine green (ICG) near-infrared fluorescence (NIF) imaging capabilities for biliary ductal identification. At our institution, ICG with NIF is not readily available during laparoscopy. Furthermore, the Xi platform’s enhanced wrist articulation offered improved maneuverability compared to laparoscopy, facilitating a safer minimally invasive cholecystectomy. Once the robot is docked, the surgeon sits at the console, which adds not only the improved ergonomics but also the “mirror image” anatomy, eliminating unnecessary reconfiguring of where the assistant and operating surgeon need to stand if performing the procedure laparoscopically. The dual console also provided excellent teaching and supervision opportunities. The robotic arm’s precision and ability to maintain consistent retraction improved accuracy and reduced surgeon fatigue. These factors supported the decision to proceed robotically for the safest and most effective approach. Preoperative CT and MRCP showed no vascular or biliary anomalies, and referral to a hepatopancreatobiliary surgeon was not indicated.
Given the patient’s SIT anatomy and prior hysterectomy, Veress needle entry was performed in the right upper quadrant. Four 8mm robotic trocars were placed, and the patient was positioned in reverse Trendelenburg with the left side up. The Xi robot was docked (Figure 2). Laparoscopic entry confirmed the right-sided heart and the left upper quadrant location of the liver and gallbladder (Figure 3). ProGrasp and Cadiere forceps were used for gallbladder retraction, and hook cautery for dissection (Figure 4). The cystic duct was identified, and dissection proceeded superior to the sulcus of Rouviere (Figure 5). ICG with NIF imaging confirmed the relationship between the cystic duct and common bile duct (Figure 6). The cystic artery (anterior and posterior branches) and cystic duct were clipped and transected. The gallbladder was completely dissected from the liver bed, and the gallbladder fossa was irrigated, confirming hemostasis and absence of bile leak (Figure 7). The gallbladder was retrieved through the umbilical port site using an Endocatch bag. The pneumoperitoneum was evacuated, and all port sites were closed.
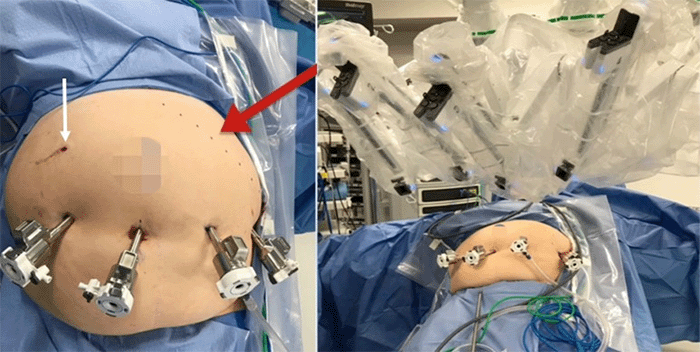
Figure 2. Initial Surgical Steps. Published with Permission
Right upper quadrant Veress needle insertion (white arrow); planned left subcostal incision line for potential open conversion (red arrow); robotic docking
Figure 3. Intraoperative Anatomy. Published with Permission
Stomach in the right upper quadrant (black arrow); liver and gallbladder in the left upper quadrant (white arrows)
Figure 4. Dissection Technique. Published with Permission
Infundibular approach with medial and lateral peritoneal dissection
Figure 5. Key Anatomical Landmarks. Published with Permission
Sulcus of Rouvière (white arrow); cystic duct (black arrow)
Figure 6. Critical View of Safety. Published with Permission
Cystic duct and common bile duct junction (white arrow); Sulcus of Rouvière (black arrow)
Figure 7. Completion of Cholecystectomy. Published with Permission
Cystic duct and cystic artery clipped and transected (white arrows); gallbladder removed from the cystic plate
The patient was discharged on postoperative day two and remained asymptomatic at one-month and one-year follow-up. Pathology revealed acute on chronic cholecystitis and cholelithiasis.
Discussion
This report details our experience and the technical aspects of robotic cholecystectomy in a patient with situs inversus totalis (SIT). Prior reports of robotic cholecystectomy in SIT include three cases for chronic cholecystitis4 and biliary colic,5 one of which was in a patient with Kartagener’s syndrome presenting with recurrent biliary colic.6 Another report describes robotic cholecystectomy during giant hiatal hernia repair in a patient with situs inversus partialis (without dextrocardia).7 To our knowledge, this is the first reported case of robotic cholecystectomy using the Xi platform in a patient with SIT presenting with gallstone pancreatitis.
Due to a previous midline laparotomy incision, umbilical Veress needle entry and open Hasson entry were deemed unsafe. Pneumoperitoneum was established via Veress needle insertion at a “mirror” Palmer’s point in the right subcostal region along the midclavicular line, given the right upper quadrant location of the stomach and spleen. The Veress needle was replaced with a 5mm laparoscopic trocar, and an 8mm robotic trocar was placed 10 cm to the right of the umbilicus. After adhesiolysis, three additional 8mm trocars were placed at the umbilicus and on the left side of the abdomen. The patient’s arms were not tucked. Following reverse Trendelenburg positioning (left side up) and left-sided robotic docking, hook cautery was inserted through the right-sided trocar, and a 30-degree 8mm angled robotic scope was placed at the umbilicus. ProGrasp forceps (left hand) and Cardiere forceps (right hand) were used through the left-sided ports for cephalad fundus retraction and infundibulum retraction, respectively. The hook cautery (right-sided port) was controlled by the surgeon’s left hand. The Xi robotic platform facilitated right-handed dissection using the left hand, requiring only one instrument exchange (hook cautery for Cardiere forceps). The initially placed right upper quadrant 5mm trocar was not used for dissection.
Intraoperative cholangiography (ICG) with near-infrared fluorescence (NIF) was used to confirm the relationship between the gallbladder, cystic duct, and common bile duct, in addition to achieving the critical view of safety. Given the altered anatomy, this adjunct was deemed essential for optimizing safety. Console time was 90 minutes (including 20 minutes for adhesiolysis), compared to operative times of 50 and 221 minutes reported in the literature.4,5
Conclusion
Gallstone pancreatitis in the setting of SIT is uncommon, and cholecystectomy is technically challenging due to the unusual anatomy. Cholecystectomy using the Xi robotic platform can be performed safely and effectively in a patients with SIT.
Lessons Learned
In this patient, “mirror” Palmer’s point Veress needle access in the right upper quadrant at the midclavicular line provided safe entry, avoiding periumbilical adhesions. The 8mm robotic trocar placed off-midline on the right side of the umbilicus facilitated adhesiolysis and prevented potential injury from initial umbilical entry. Robotic cholecystectomy using the Xi platform was safe and effective in this patient with SIT. The robotic platform offered the advantages of “open-like” surgery in a minimally invasive fashion and allowed for ICG with NIF to confirm anatomy and identify the cystic duct and its relationship with the common bile duct.
Department of Surgery, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, PA 19107
Department of Surgery, Division of Acute Care Surgery, Thomas Jefferson University, Philadelphia, PA 19107
Corresponding Author
Luke T. Meredith, MD Thomas Jefferson University Hospital 1015 Walnut Street, Ste. 613 Philadelphia, PA 19107 Email: lxm460@jefferson.edu
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding/Support
The authors have no relevant financial relationships or in-kind support to disclose.
Received: August 16, 2023 Revision received: January 4, 2024 Accepted: January 24, 2024
References
Campos L, Sipes E. Laparoscopic cholecystectomy in a 39-year-old female with situs inversus. J Laparoendosc Surg. 1991;1(2):123-126. doi:10.1089/lps.1991.1.123
Enciu O, Toma EA, Tulin A, Georgescu DE, Miron A. Look beyond the Mirror: Laparoscopic Cholecystectomy in Situs Inversus Totalis-A Systematic Review and Meta-Analysis (and Report of New Technique). Diagnostics (Basel). 2022;12(5):1265. Published 2022 May 19. doi:10.3390/diagnostics12051265
Ponce Leon F, Fiorencio MH, Leal CP, Santos AR. Laparoscopic cholecystectomy in a patient with situs inversus totalis after videolaparoscopic sleeve-Case report. Int J Surg Case Rep. 2020;71:202-204. doi:10.1016/j.ijscr.2020.04.045
Meghana SS, Bala Krishna A, Syama Sundara Rao T, Raju BV, Nayak SR. Robotic cholecystectomy in a case of situs inversus totalis. Ann Robot Innov Surg. 2023 May;4(1):6-11. doi:10.37007/aris.2023.4.1.6
Magarinos J, Fajardo R, Attiya R. Use of Robotic Surgery Platform for Cholecystectomy in a Patient with Situs Inversus Totalis. Videoscopy. 2022;[Epub ahead of print]. doi:10.1089/vor.2022.0036
Muriel P, Escartín A, González ML, Olsina JJ. Robotic cholecystectomy in situs inversus totalis. Colecistectomía robótica en situs inversus totalis. Cir Esp (Engl Ed). 2020;98(9):554. doi:10.1016/j.ciresp.2020.03.020
Ceccarelli G, Romano A, Esposito G, et al. Robot-assisted Toupet fundoplication and associated cholecystectomy in symptomatic giant hiatal hernia with situs viscerum inversus-A case report and literature review. Int J Surg Case Rep. 2019;60:371-375. doi:10.1016/j.ijscr.2019.06.038