Abstract
Background
Malignant melanoma metastasizing to the gallbladder is an exceedingly rare occurrence, with such lesions often being asymptomatic and discovered incidentally. This report describes a case of metastatic melanoma involving both the gallbladder and the small intestine, highlighting the diagnostic and surgical considerations.
Summary
We present a 74-year-old asymptomatic male with a history of cutaneous malignant melanoma, which had been resected nine years prior. Abdominal ultrasound and magnetic resonance imaging (MRI) identified an incidental gallbladder mass suspicious for primary gallbladder adenocarcinoma. The patient subsequently underwent an en bloc cholecystectomy, partial hepatectomy (segments IVb/V), and portal lymphadenectomy. During abdominal exploration, a fixed, intraluminal jejunal mass was palpated and contemporaneously resected. Immunohistochemical analysis of both the gallbladder and jejunal specimens confirmed metastatic malignant melanoma.
Conclusion
This case underscores that while infrequent, metastatic melanoma should be considered in the differential diagnosis of a new gallbladder mass in patients with a prior history of cutaneous melanoma. Furthermore, it emphasizes the importance of meticulous intraoperative exploration and palpation of the entire gastrointestinal tract due to the potential for synchronous, clinically occult sites of metastasis.
Key Words
gallbladder melanoma; metastatic melanoma; small intestine melanoma
Case Description
A 74-year-old male with a history of resected superficial spreading malignant melanoma presented to our clinic following the incidental discovery of a gallbladder mass. Nine years prior, he was diagnosed with a superficial spreading malignant melanoma of the left upper arm (Breslow depth 0.8 mm, Clark’s level IV, T1b) following a shave biopsy that revealed positive peripheral margins. Wide local excision (WLE) and sentinel lymph node biopsy (SLNB) were recommended; however, the patient elected for WLE only, declining SLNB due to concerns regarding lymphedema and general anesthesia. The subsequent WLE specimen showed no residual melanoma or dysplastic nevi. In lieu of SLNB, he underwent surveillance with cutaneous and axillary lymph node ultrasounds and had regular dermatological follow-up, with no new or recurrent cutaneous lesions identified since his initial treatment.
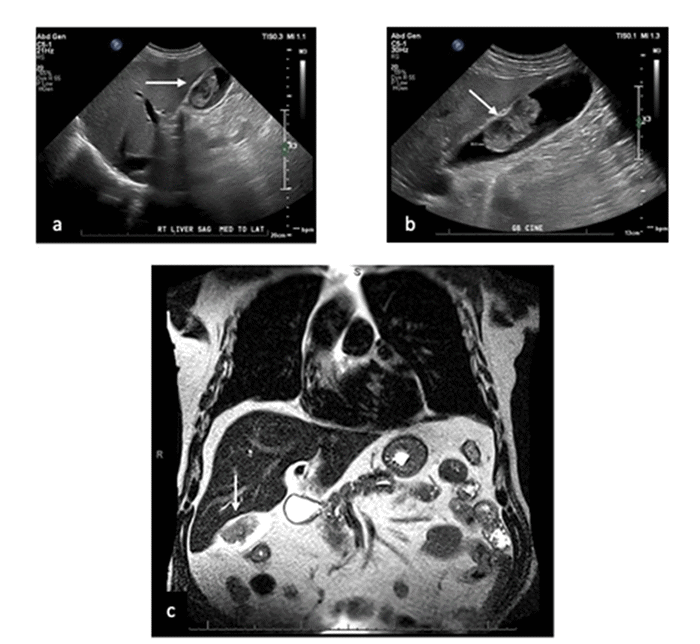
In May 2022, the patient developed a COVID-19 infection and was treated with nirmatrelvir/ritonavir, which led to a transient elevation in his liver function tests. His physical examination at that time was unremarkable, without scleral or cutaneous icterus, hepatosplenomegaly, or abdominal pain or masses. An abdominal ultrasound performed to evaluate the liver enzymes incidentally demonstrated a gallbladder mass. Subsequent magnetic resonance imaging (MRI) of the abdomen further characterized this as a 5.0 × 2.6 × 4.3 cm intraluminal mass exhibiting T2 hypointensity, marked diffusion restriction, and progressive, patchy contrast enhancement, without evidence of direct liver invasion. An enhancing cystic duct lymph node was also noted (Figure 1). These findings were suspicious for a primary gallbladder adenocarcinoma. Staging computed tomography (CT) of the chest, abdomen, and pelvis revealed no other evidence of distant metastatic disease.
Figure 1. Preoperative Imaging of Gallbladder Mass. Published with Permission
Given the suspicion for gallbladder cancer, the patient underwent a scheduled open cholecystectomy with en bloc partial hepatectomy (segments IVb/V) and portal lymphadenectomy. He tolerated the procedure well, and intraoperative frozen section analysis of the cystic duct and hepatic resection margins was negative for malignancy. During abdominal exploration, a 2 cm fixed, polypoid, intraluminal jejunal mass was unexpectedly palpated. This was resected within a 5 cm segment of jejunum, and intestinal continuity was restored with a hand-sewn side-to-side jejunojejunostomy. Frozen section of the jejunal mass was suspicious for malignancy. The patient’s postoperative course was uneventful, and he was discharged home on postoperative day three.
Final pathological analysis confirmed that both the 5.0 × 2.6 × 4.3 cm gallbladder mass and the 2.2 cm jejunal mass were metastatic melanoma. All surgical margins were negative, and 0 of 2 resected lymph nodes were positive for malignancy (Figures 2, 3). Molecular profiling of the tumor tissue (Table 1) revealed wild-type KIT and BRAF genes, but an NRAS mutation at codon 61 (Q61) was identified. Additionally, a monoallelic deletion of EWSR1 was detected, though without evidence of rearrangement; the significance of this EWSR1 alteration in melanoma is currently unclear, as it is more commonly associated with sarcomas. NRAS mutations are present in approximately 15-20% of melanomas and are generally associated with a more aggressive clinical course and poorer prognosis compared to non-NRAS-mutant melanomas.
Figure 2. Histopathological Features of Metastatic Melanoma. Published with Permission
Postoperative staging MRI of the brain revealed two small hemorrhagic metastases, measuring 3 mm and 2 mm, in the right and left frontal lobes, respectively. The patient was evaluated by medical oncology and initiated on combination immunotherapy with nivolumab/relatlimab (anti-PD-1/anti-LAG-3), completing three infusions to date. He was also referred to neurosurgery and radiation oncology and underwent Gamma Knife radiosurgery for the brain metastases in September 2022. During this assessment, an additional 1.6 cm dural-based lesion, suspicious for either metastasis or meningioma, was identified, and short-interval imaging follow-up was planned. A repeat brain MRI in November 2022 demonstrated a decrease in the size of the irradiated frontal lobe lesions and stability of the dural lesion. The patient is currently responding well to treatment and continues under multidisciplinary care.
Discussion
Melanoma, an aggressive malignancy originating from melanocytes, exhibits a high propensity for metastatic dissemination via hematogenous and lymphatic routes, potentially affecting virtually any organ.1-3 While cutaneous melanoma is the most common form, arising from epidermal melanocytes, it accounts for a smaller percentage of all skin cancers but carries significant mortality risk due to its metastatic potential. The gastrointestinal (GI) tract is a frequent site for melanoma metastasis; although clinically evident GI involvement occurs in only 5-10% of patients, postmortem studies reveal a much higher incidence, approaching 60%.4 Common sites within the GI tract include the small bowel (51-71%), stomach (27%), large intestine (22%), and esophagus (5%).5 Metastatic involvement of the gallbladder, however, is rarely described in clinical practice. A study by Marone et al. reviewing 1684 cutaneous melanoma patients identified GI metastases in 30 individuals, with only one case involving the gallbladder.2 In stark contrast, autopsy series indicate a gallbladder metastasis prevalence of 15-20% in patients with disseminated melanoma, highlighting the often clinically occult nature of these lesions.6
The discrepancy between clinical and autopsy detection rates for gallbladder melanoma metastases is largely attributed to their frequently asymptomatic presentation, with lesions often discovered incidentally, as in the current case. When symptomatic, patients may present with obstructive jaundice due to biliary tree compression or symptoms mimicking cholecystitis, such as right upper quadrant pain, nausea, and vomiting. Epidemiologically, a review by Bangeas et al. analyzing 57 articles on gallbladder melanoma found a male predominance (3:1 ratio) and a mean age at diagnosis of 55 (±14) years, with primary tumors originating from various cutaneous sites.7 The interval between primary melanoma diagnosis and the appearance of gallbladder metastases is highly variable. Katz et al., reporting on 13 cases from Memorial Sloan-Kettering Cancer Center, noted a median interval of 39 months (range 0 to 248 months).8 Our patient presented with gallbladder metastasis nine years (108 months) after his initial cutaneous melanoma diagnosis, underscoring the potential for very late recurrence.
The diagnostic workup for an incidentally discovered gallbladder mass typically commences with abdominal ultrasonography, which may reveal a thickened gallbladder wall or intraluminal hyperechoic masses, potentially with Doppler flow signals.9 However, ultrasound is operator-dependent and may miss small lesions. Cross-sectional imaging with CT, MRI, or positron emission tomography (PET) offers more reliable and detailed characterization.10 In our patient, ultrasound prompted further investigation, and MRI delineated features initially suspicious for a primary gallbladder adenocarcinoma. The differential diagnosis for a gallbladder mass is broad, including benign polyps (cholesterol, adenomyomatous), adenomas, primary gallbladder cancers (adenocarcinoma being the most common, followed by less frequent histological subtypes like papillary or mucinous carcinoma), and metastases from other primaries such as renal cell carcinoma, or direct invasion from hepatocellular carcinoma.11 Crucially, metastatic melanoma must be considered in any patient with a new gallbladder lesion and a history of melanoma, irrespective of the time elapsed since primary tumor resection.
Given the rarity of metastatic melanoma to the gallbladder, standardized management guidelines are lacking. Surgical resection is generally accepted as the mainstay of therapy and can offer palliative benefit, local disease control, and potentially prolong survival, even in the context of disseminated disease.8,12 An open surgical approach, as employed in our patient, is often recommended over laparoscopy to facilitate thorough abdominal exploration and palpation of the entire GI tract for previously undetected synchronous metastases.13 This proved beneficial in our case, leading to the discovery and resection of an occult jejunal metastasis not visualized on preoperative imaging. For select patients with oligometastatic disease and factors portending a poor prognosis, neoadjuvant systemic therapy may be considered to assess treatment response and potentially downstage disease before surgery.
Systemic therapy for metastatic melanoma has evolved significantly, driven by an understanding of molecular pathogenesis. Treatment selection is heavily influenced by the tumor’s mutational profile, including alterations in BRAF, NRAS, and KIT genes. For tumors harboring a BRAF V600 mutation (approximately 40% of melanomas), combination therapy with BRAF and MEK inhibitors (e.g., dabrafenib/trametinib) is a standard approach. In patients with NRAS-mutated melanomas, such as ours, immune checkpoint inhibitors are typically first-line treatment, with cytotoxic chemotherapy (e.g., carboplatin/paclitaxel, dacarbazine, temozolomide) reserved for subsequent lines. For KIT-mutated melanomas, anti-PD-1 immunotherapy is favored, with KIT inhibitors like imatinib also playing a role, particularly in ongoing trials. BRAF wild-type tumors are generally treated with PD-1 inhibitors, such as nivolumab or pembrolizumab, or combination immunotherapy like nivolumab/relatlimab as used in our patient.13,14 Adjuvant therapy post-resection is frequently recommended for stage III and IV melanoma due to the high risk of recurrence, with the choice of agent guided by tumor characteristics, mutational status, treatment-related risks, and patient factors.
Despite therapeutic advances, the prognosis for metastatic melanoma to the gallbladder remains poor, reflecting the aggressive nature of the disease and its tendency for late or asymptomatic presentation at an advanced stage. Reported median survival following diagnosis of gallbladder metastasis varies widely, typically ranging from 1 to 12 months, largely dependent on the presence and extent of concurrent multifocal metastatic disease.8
Conclusion
Metastatic melanoma involving the gallbladder is an uncommon clinical entity, often presenting asymptomatically and thus typically diagnosed at an advanced stage, which inherently carries a guarded prognosis. It is therefore imperative for clinicians to maintain a high index of suspicion for metastatic melanoma in any patient presenting with a new gallbladder mass who has a prior history of cutaneous melanoma; this underscores the importance of a meticulous patient history, irrespective of the disease-free interval since the primary tumor diagnosis.
Lessons Learned
When surgical resection of suspected or confirmed gallbladder melanoma metastases is undertaken, an open approach is strongly advocated. This strategy facilitates a comprehensive intraoperative exploration, including careful inspection and palpation of the entire gastrointestinal tract. Such thorough examination is critical due to melanoma’s propensity for multifocal gastrointestinal involvement, which may include clinically occult synchronous metastases not detected by preoperative imaging, as demonstrated in the present case. Identifying all sites of disease is crucial for accurate staging and informs optimal subsequent oncologic management.
Authors
Rama Ma; Kittle Hb; Lynch Lb; Lee Sc; Lavu Hb
Author Affiliations
- Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, PA 19107
- Department of Surgery, Thomas Jefferson University Hospital, Philadelphia, PA 19107
- Department of Pathology and Genomic Medicine, Thomas Jefferson University Hospital, Philadelphia, PA 19107
Corresponding Author
Harish Lavu, MD, FACS
Department of Surgery
Thomas Jefferson University
1015 Walnut Street
Ste. 620
Philadelphia, PA 19107
Email: harish.lavu@jefferson.edu
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding/Support
The authors have no relevant financial relationships or in-kind support to disclose.
Received: November 9, 2023
Revision received: January 23, 2024
Accepted: February 28, 2024
References
- Patel D, Sohrawardy S, Sedhai YR, et al. Metastatic cutaneous melanoma of the gallbladder. Case Rep Gastrointest Med. 2017;2017:8532379. doi:10.1155/2017/8532379
- Marone U, Caracò C, Losito S, et al. Laparoscopic cholecystectomy for melanoma metastatic to the gallbladder: is it an adequate surgical procedure? Report of a case and review of the literature. World J Surg Oncol. 2007;5:141. doi:10.1186/1477-7819-5-141
- Di Buono G, Maienza E, Rinaldi G, Buscemi S, Romano G, Agrusa A. Malignant metastatic melanoma to the gallbladder: report of a peculiar case. Int J Surg Case Rep. 2020;77S:S37-S39. doi:10.1016/j.ijscr.2020.08.044
- Kohoutova D, Worku D, Aziz H, Teare J, Weir J, Larkin J. Malignant melanoma of the gastrointestinal tract: symptoms, diagnosis, and current treatment options. Cells. 2021;10(2):327. doi:10.3390/cells10020327
- López RG, Santomé PM, Porto EI, et al. Intestinal perforation due to cutaneous malignant melanoma mestastatic implants. Rev Esp Enferm Dig. 2011;103(7):386-388. doi:10.4321/s1130-01082011000700014
- Gupta TD, Brasfield R. Metastatic melanoma: a clinicopathological study. Cancer. 1964;17(10):1323-1339. doi:10.1002/1097-0142(196410)17:10<1323::aid-cncr2820171015>3.0.co;2-n
- Bangeas PI, Bekiaridou A, Tsolakidis A, et al. Role of minimally invasive surgery in the treatment of gallbladder metastatic melanoma: a review of the literature and a case report. Cancer Rep (Hoboken). 2022;5(7):e1549. doi:10.1002/cnr2.1549
- Katz SC, Bowne WB, Wolchok JD, Busam KJ, Jaques DP, Coit DG. Surgical management of melanoma of the gallbladder: a report of 13 cases and review of the literature. Am J Surg. 2007;193(4):493-497. doi:10.1016/j.amjsurg.2006.06.033
- Vesnin AG, Semenov II, Negustorov IuF, Anisimov VV, Turkevich EA. [Ultrasound diagnosis of melanoma metastasis into the gallbladder]. Vopr Onkol. 1999;45(6):690-692.
- Rehani B, Strohmeyer P, Jacobs M, Mantil J. Gallbladder metastasis from malignant melanoma: diagnosis with FDG PET/CT. Clin Nucl Med. 2006;31(12):812-813. doi:10.1097/01.rlu.0000246860.97977.e1
- Henson DE, Albores-Saavedra J, Corle D. Carcinoma of the gallbladder. Histologic types, stage of disease, grade, and survival rates. Cancer. 1992;70(6):1493-1497. doi:10.1002/1097-0142(19920915)70:6<1493::aid-cncr2820700608>3.0.co;2-u
- Giannini I, Cutrignelli DA, Resta L, Gentile A, Vincenti L. Metastatic melanoma of the gallbladder: report of two cases and a review of the literature. Clin Exp Med. 2016;16(3):295-300. doi:10.1007/s10238-015-0353-6
- Christou D, Katodritis N, Decatris MP, et al. Melanoma of the gallbladder: appropriate surgical management and review of the literature. Clin Case Rep. 2014;2(6):313-318. doi:10.1002/ccr3.121
- Wada-Ohno M, Ito T, Furue M. Adjuvant therapy for melanoma. Curr Treat Options Oncol. 2019;20(8):63. doi:10.1007/s11864-019-0666-x