Abstract
Background
This case report describes a complex, multidisciplinary surgical approach required to repair a rare strangulated small bowel diaphragmatic hernia in a patient with a history of gastric bypass surgery and hiatal hernia repair.
Summary
A 67-year-old woman, three months status post-robotic Roux-en-Y gastric bypass (RYGB) and concurrent hiatal hernia repair, presented to the emergency department with severe abdominal pain, shortness of breath, and right-sided chest pain. She exhibited visible distress, tachycardia, hypertension, tachypnea, and impending respiratory failure. Abnormal lab results included leukocytosis, hyperglycemia, elevated lipase, and lactic acidosis. A CT scan revealed a large right-sided diaphragmatic hernia containing small bowel with signs of ischemia and compressive signs on the right lung. The CT scan also suggested pancreatitis. Due to respiratory distress, the patient underwent emergency surgery following fluid resuscitation.
Laparoscopy revealed small bowel herniation through the diaphragmatic hiatus. Attempts at laparoscopic hernia reduction were unsuccessful, leading to a laparotomy. However, due to the extent of herniated bowel and the size of the hernia defect, abdominal reduction was also unsuccessful. Consequently, a thoracic surgeon was consulted to perform a thoracotomy. The right thoracic cavity was found to contain strangulated and necrotic small bowel. Given the patient's hemodynamic instability, a damage control surgery (DCS) approach was implemented in three phases. First, the necrotic portion of the Roux limb was resected, and the thoracotomy was closed with a thoracostomy tube. The abdominal wall was temporarily closed, leaving the patient in discontinuity. Second, the patient was transferred to the intensive care unit for resuscitation. Third, the patient returned to the operating room for definitive repair. The patient's gastric pouch and remaining small bowel were viable. The original gastric bypass was reversed via gastrogastrostomy, and a feeding jejunostomy was created using the remaining healthy Roux limb. The patient was discharged after an uneventful recovery and remained asymptomatic at 18-month follow-up.
Conclusion
This case underscores the importance of a high index of suspicion for post-bariatric surgery hiatal hernias, particularly in patients presenting with rapid-onset symptoms. A multidisciplinary surgical approach and standardized operative procedures are crucial for successful management. Although the rarity of such cases hinders the development of a unified management strategy, collaborative efforts toward standardization are imperative.
Key Words
hiatal hernia; strangulated hernia; Roux-en-Y; gastric bypass
Case Description
A 67-year-old female presented to the emergency department with abdominal pain, shortness of breath, and right-sided chest pain. The abdominal pain began upon awakening and progressively worsened throughout the day. The patient reported an intense urge to vomit but was unable to do so. One hour prior to arrival, she experienced sudden onset cramping lower abdominal pain and shortness of breath, prompting her to seek medical attention. Her medical comorbidities include hypertension, obesity, Crohn's disease, hyperlipidemia, hypothyroidism, obstructive sleep apnea requiring continuous positive airway pressure, and non-insulin-dependent type 2 diabetes mellitus. Approximately three months prior to this presentation, she underwent a robotic Roux-en-Y gastric bypass (RYGB), creating a 125 cm antecolic Roux limb. Concomitantly, a primary posterior crural repair was performed for a known large hiatal hernia containing approximately half the stomach in the chest. The patient had a three-month postoperative follow-up in the bariatric surgery clinic only three days prior to this presentation, reporting good compliance with bariatric protocols and no complications.
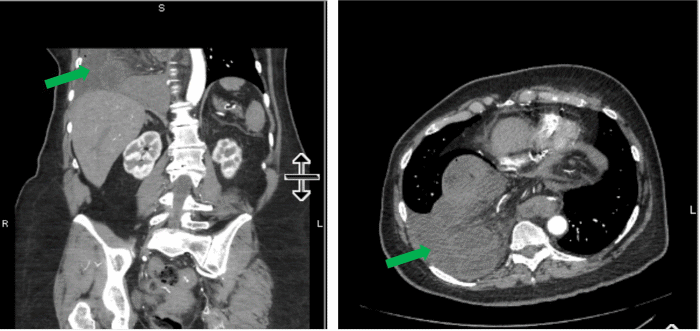
Upon presentation to the emergency department, clinical exam revealed a mildly distressed patient with a temperature of 36.8°C, mild tachycardia (106 beats per minute), hypertension (145/121 mmHg), respiratory rate of 21 breaths per minute with oxygen saturation of 98%, clear lung auscultation bilaterally, and abdominal pain disproportionate to palpation. Laboratory tests showed leukocytosis, hyperglycemia, elevated lipase, and lactic acidosis. CT of the abdomen and pelvis demonstrated a large right-sided diaphragmatic hernia containing multiple loops of dilated small bowel extending into the right thoracic cavity and lung base, with surrounding fluid, wall thickening, and possible pneumatosis, suggestive of ischemic bowel. Due to CT scan windowing, the full extent of herniation could not be visualized. Additionally, fat stranding of the pancreatic tail was observed, suggestive of pancreatitis (Figure 1). Given the presenting symptoms of shortness of breath and abdominal pain, and the concern for strangulated bowel, the patient was taken emergently to the operating room.
Figure 1. CT Imaging of Right Diaphragmatic Hernia. Published with Permission
Preoperatively, the patient underwent fluid resuscitation and received prophylactic antibiotics and venous thromboembolism prophylaxis. Surgery was initially performed laparoscopically in the left upper quadrant. A small diaphragmatic slit near the inferior vena cava was created. However, attempts to reduce the hernia back into the abdomen were unsuccessful. Consequently, conversion to laparotomy was performed via an epigastric midline incision from the xiphoid process to the umbilicus. The diaphragm was further divided, but this resulted in only minimal reduction of the hernia contents. At this point, cardiothoracic surgery was consulted intraoperatively, and a right-sided thoracotomy was performed. The patient's endotracheal tube was exchanged for a double-lumen endobronchial tube to facilitate right thoracic cavity exposure by collapsing the right lung and using single left-lung ventilation. Upon exploration, several feet of ischemic and necrotic-appearing small bowel were observed in the right chest (Figure 2). Under direct visualization, the diaphragm was divided in a posterolateral radial fashion to enlarge the esophageal hiatus, facilitating reduction of the herniated bowel back into the peritoneal cavity, with additional traction applied through the open laparotomy incision. Right lung reinflation and ventilation were resumed without difficulty. The diaphragmatic hernia was then closed with interrupted 0 Nurolon sutures. Due to the extended operative time, damage control surgery (DCS) was performed. The first phase of DCS included (1) resection of approximately 130 cm of necrotic Roux limb from the gastrojejunal anastomosis to 10 cm proximal to the jejunojejunal anastomosis, leaving an estimated 160 cm of small bowel, (2) insertion of a right thoracostomy tube with closure of the thoracotomy, and (3) temporary abdominal wall closure using a negative pressure wound therapy device (e.g., ABThera wound vacuum therapy). The patient was left in discontinuity, and a subsequent procedure was planned for reversal of her gastric bypass and feeding jejunostomy. The second phase of DCS involved transferring the patient to the ICU for further resuscitation, where she was awake, alert, and following commands as sedation was weaned.
Figure 2. Intraoperative View of Ischemic Small Bowel in Right Thorax. Published with Permission
The third phase of DCS (definitive repair) was performed two days later. The patient was taken to the operating room, where the ABThera wound vacuum was removed, and the gastric pouch and remnant were found to be healthy and viable. The remaining small bowel was examined and also found to be viable. An esophagogastroduodenoscopy (EGD) was performed to confirm mucosal lining integrity. At this point, the decision was made to proceed with reversal of the gastric bypass via gastrogastrostomy. A gastrogastric anastomosis between the gastric pouch and remnant was created using a 25 EEA stapler. The gastrotomy was also closed with the stapler. A repeat intraoperative EGD was performed, which resulted in a negative leak test. A nasogastric tube was inserted distal to the staple line, and a Jackson-Pratt drain was placed. The remaining healthy Roux limb was brought to the abdominal wall as a Stamm feeding jejunostomy. The abdominal fascia and skin were then closed.
The patient was extubated on postoperative day (POD) 1 and started on jejunostomy tube feeds. Oral analgesia was initiated on POD 2, and the patient was fully transitioned off intravenous narcotics by POD 4. The patient's bowel function returned, and she was eventually transitioned to oral intake while weaning jejunostomy tube feeds. On POD 4, the patient was afebrile and had vital signs within normal limits; however, blood tests revealed rising leukocytosis. A CT scan of the chest, abdomen, and pelvis showed a moderate left upper quadrant fluid collection suspicious for seroma. Interventional radiology was consulted for fluid drainage. A left upper quadrant ultrasound, however, demonstrated fluid interposed between the spleen, multiple small bowel loops, and the left kidney, without a safe window for percutaneous drainage. Therefore, the fluid collection was presumed to be infected with gram-negative and anaerobic enteric bacteria and was treated with ceftriaxone and metronidazole. Leukocytosis was completely resolved by POD 8, and no further imaging was required. The patient was deemed stable for discharge home on POD 9. The patient was seen regularly in follow-up visits up to 18 months after initial presentation and reported overall well-being. Although her original gastric bypass was reversed, the patient continued medical weight management and maintained a stable weight for at least 20 months after initial presentation.
Discussion
A hiatal hernia is a type of hernia in which a portion of the gastrointestinal tract protudes through the diaphragmatic hiatus into the thoracic cavity. Hiatal hernias are classified into four types based on the anatomical disruption: sliding, paraesophageal, combined paraesophageal and sliding, and hernias with additional abdominal organ involvement.1 The etiology of hiatal hernias is most commonly acquired, but congenital factors, such as diaphragmatic muscle weakness, may also contribute. These hernias are associated with increasing age and factors that elevate intra-abdominal pressure, including obesity, pregnancy, chronic obstructive pulmonary disease, and trauma.
Hiatal hernias are highly prevalent, occurring in over 55% of individuals older than 50 years.2 They represent a significant postoperative complication following bariatric surgery, often due to the disruption of conventional attachments of the spleen and adjacent structures, predisposing to foregut slippage. In patients undergoing weight loss surgery, the incidence of hiatal hernias can reach up to 40%, manifesting even up to 16 years after the initial procedure.3 Post-bariatric surgery hernias represent a significant complication and often present with a constellation of symptoms termed "BARF" symptoms: bloating, abdominal pain, reflux or regurgitation, and food intolerance.4,5 However, many of these symptoms can also result from poor eating behaviors observed in bariatric patients, such as overeating, rapid swallowing, inadequate chewing, and drinking fluids with meals. Therefore, a high index of suspicion for hernia is crucial during bariatric surgery follow-up visits. Additionally, atypical presentations of postoperative hiatal hernias have been documented, including severe pain radiating to the jaw, left shoulder, and midscapular area.6 Hiatal hernia diagnosis following bariatric surgery is complex, further complicated by overlapping symptoms, yet operative repair typically resolves residual symptoms.6,7
Hiatal hernias that contain the Roux limb and cause obstruction are extremely rare, with only six cases reported to our knowledge, and in none of those cases was the Roux limb necrotic.8–13 Consequently, there are no current consensus guidelines on the management of this rare but serious complication. In the case presented here, the diaphragmatic hernia was successfully closed using interrupted sutures alone, with no evidence of recurrence within 20 months. In another case series of hiatal hernia repair following bariatric surgery, all repairs were performed laparoscopically and utilized bioabsorbable mesh.3 The use of bioabsorbable mesh at the time of initial bariatric surgery has been shown to reduce the recurrence of hiatal hernias on follow-up.14 Two additional hiatal hernia repair techniques reported in the literature are a modified Nissen fundoplication and hiatoplasty utilizing the ligamentum teres hepatis. Modified Nissen fundoplication, in which a fundoplication around the gastric pouch was created using the bypassed portion of the stomach, has been successfully employed in two cases.13,15 Hiatoplasty using the ligamentum teres hepatis has been demonstrated to improve early hiatal hernia recurrence in two trials, but long-term durability remains in question.13,16,17 Overall, the scarcity of reported cases and the variety of reported repair techniques highlight the need for a unified management strategy.
Conclusion
Our patient was a 67-year-old female who presented three months following an RYGB procedure and concurrent posterior crural hiatal hernia repair with a large, right-sided diaphragmatic hernia containing a strangulated and necrotic Roux limb extending into the right thoracic cavity. While this patient experienced a favorable outcome, as evidenced by symptom resolution and the absence of recurrence at 18-month follow-up, this case underscores the critical importance of early recognition and prompt therapeutic intervention in managing this rare and potentially life-threatening complication. The unusual presentation and the need for a multi-staged approach highlight the challenges in managing these complex cases. Future research should focus on identifying predictive factors for this specific type of post-bariatric hernia and developing standardized surgical management protocols to optimize patient outcomes.
Lessons Learned
Recurrence of hiatal hernias after gastric bypass surgery is relatively common. However, herniation of the gastric pouch and Roux limb represents a rare yet severe presentation with the potential for significant morbidity. Successful management of this complex condition often necessitates a multidisciplinary surgical approach, which could be facilitated by the development of standardized operative procedures. Although the literature is sparse, current evidence demonstrates success with varied surgical techniques. Maintaining a high index of suspicion is crucial for the early detection of post-bariatric surgery hiatal hernias, as this is key to timely intervention and the prevention of catastrophic complications such as the one demonstrated in our patient.
Authors
Chen KWa; Ranat KDa; Kircher CJa,b; Elian Aa,b; Verseman SRa,b; Shebrain SAa,b
Author Affiliations
- Western Michigan University Homer Stryker M.D. School of Medicine, Kalamazoo, MI 49007
- Department of Surgery, Western Michigan University Homer Stryker M.D. School of Medicine, Kalamazoo, MI 49007
Corresponding Author
Kevin Chen
Western Michigan University Homer Stryker M.D. School of Medicine
1000 Oakland Drive
Kalamazoo, MI 49008
Email: kevin.chen@wmed.edu
Meeting Presentations
Society of American Gastrointestinal and Endoscopic Surgeons (SAGES), Montreal, Canada, March 2023
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding/Support
The authors have no relevant financial relationships or in-kind support to disclose.
Received: October 1, 2023
Revision received: January 7, 2024
Accepted: February 28, 2024
References
- Cha RR. Find out the differences by types of hiatal hernia! J Neurogastroenterol Motil. 2020;26(1):4-5. doi:10.5056/jnm19227
- Richter JE, Rubenstein JH. Presentation and epidemiology of gastroesophageal reflux disease. Gastroenterology. 2018;154(2):267-276. doi:10.1053/j.gastro.2017.07.045
- Clapp B, Vo LU, Lodeiro C, et al. Late-term hiatal hernia after gastric bypass: an emerging problem. Surg Obes Relat Dis. 2020;16(4):471-475. doi:10.1016/j.soard.2020.01.018
- Borbély Y, Kröll D, Nett PC, Moreno P, Tutuian R, Lenglinger J. Radiologic, endoscopic, and functional patterns in patients with symptomatic gastroesophageal reflux disease after Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2018;14(6):764-768. doi:10.1016/j.soard.2018.02.028
- Al-Bahri S, Murr M, Gonzalvo JP. Doctor, why do I BARF? Hiatal hernias as a cause of chronic bloating, abdominal pain, reflux, regurgitation and food intolerance in patients with a history of bariatric surgery. Surg Obes Relat Dis. 2016;12(7):S176-S177. doi:10.1016/j.soard.2016.08.315
- Flanagin BA, Mitchell MT, Thistlethwaite WA, Alverdy JC. Diagnosis and treatment of atypical presentations of hiatal hernia following bariatric surgery. Obes Surg. 2010;20(3):386-392. doi:10.1007/s11695-009-0013-6
- Golas A, El-Attrache BFM, Jorge J, Dietrick J, Gonzalvo JP, Murr MM. Repair of post-bariatric surgery, recurrent, and de novo hiatal hernias improves bloating, abdominal pain, regurgitation, and food intolerance. Surg Obes Relat Dis. 2021;17(4):683-691. doi:10.1016/j.soard.2020.12.006
- Yagnik Pandya, Donald Hess. Hiatal Hernias Causing Post Operative Bowel Obstruction Following Roun En Y Gastric Bypass - SAGES Abstract Archives. SAGES. Published July 19, 2019. Accessed September 28, 2023. https://www.sages.org/meetings/annual-meeting/abstracts-archive/hiatal-hernias-causing-post-operative-bowel-obstruction-following-roun-en-y-gastric-bypass/
- Borg CM, Katz-Summercorn A, Adamo M. Acute diaphragmatic herniation as cause of small bowel obstruction after gastric bypass. Surg Obes Relat Dis. 2011;7(4):e6-e8. doi:10.1016/j.soard.2010.07.010
- Caceres M, Eid GM, McCloskey CA. Recurrent paraesophageal hernia presenting as obstruction of Roux limb after Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2010;6(2):197-199. doi:10.1016/j.soard.2009.10.008
- Cardaci MB, Keuleneer RD, Massaarani F. Hiatal hernia containing the alimentary limb and the gastric pouch: a rare cause of small bowel obstruction after Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2017;13(11):1929-1931. doi:10.1016/j.soard.2017.08.014
- Nance ME, Shapera E, Wheeler AA. Type IV hiatal hernia containing the gastric pouch and proximal Roux limb: a rare cause of bowel obstruction following Roux-en-Y bypass surgery. Cureus. 2020;12(8):e10132. doi:10.7759/cureus.10132
- Thomopoulos T, FitzGerald M, Mantziari S, Demartines N, Suter M. Management of a late-term hiatal hernia with intrathoracic pouch migration after Roux-en-Y gastric bypass. Obes Surg. 2022;32(3):957-958. doi:10.1007/s11695-021-05881-1
- Clapp B, Kara AM, Nguyen-Lee PJ, et al. Does the use of bioabsorbable mesh for hiatal hernia repair at the time of bariatric surgery reduce recurrence rates? A meta-analysis. Surg Obes Relat Dis. 2022;18(12):1407-1415. doi:10.1016/j.soard.2022.08.004
- Kawahara NT, Alster C, Maluf-Filho F, Polara W, Campos GM, Poli-de-Figueiredo LF. Modified Nissen fundoplication: laparoscopic antireflux surgery after Roux-en-Y gastric bypass for obesity. Clinics (Sao Paulo). 2012;67(5):531-533. doi:10.6061/clinics/2012(05)23
- Runkel A, Scheffel O, Chiappetta S, Marjanovic G, Runkel N. Hiatoplasty for intrathoracic gastric migration associated with one anastomosis gastric bypass (OAGB). Obes Surg. 2020;30(12):4986-4994. doi:10.1007/s11695-020-04886-6
- Runkel A, Scheffel O, Marjanovic G, Runkel N. The new interest of bariatric surgeons in the old ligamentum teres hepatis. Obes Surg. 2020;30(11):4592-4598. doi:10.1007/s11695-020-04918-1