Abstract
Background
Abdominal tuberculosis (TB) is a rare complication of pulmonary TB, often associated with immunocompromise. Due to effective public health measures and widespread antibiotic use, TB appendicitis is virtually nonexistent in developed countries. This report describes a case of abdominal TB causing recurrent appendicitis in a patient with a malignancy of unknown primary.
Summary
A 43-year-old male from Micronesia with a known history of pulmonary TB and limited English proficiency presented with melena, right lower quadrant abdominal pain, and fever. Initial workup revealed appendicitis secondary to lymphadenopathy and regional abdominal TB, along with a mass compressing the third portion of the duodenum. He was initially managed non-operatively and underwent lymph node biopsy, which demonstrated concomitant poorly differentiated carcinoma. Due to recurrent abdominal symptoms, surgical intervention with bypass and appendectomy was offered. However, the patient opted for traditional healing and subsequently died from aspiration.
Conclusion
This case highlights the importance of considering a broad differential diagnosis in vulnerable populations. While surgical intervention for TB appendicitis can be effective, it is not the primary treatment modality. This complex case required multidisciplinary collaboration and underscores the challenges in managing patients with limited access to healthcare and competing cultural beliefs.
Key Words
abdominal tuberculosis; appendicitis; malignancy of unknown primary; cultural humility
Case Description
A 43-year-old male who recently emigrated from Micronesia presented to an urban tertiary care center. The patient, who spoke limited English, reported melena, right lower quadrant abdominal pain, and fevers with chills. His medical history included pulmonary tuberculosis (TB) with a lung mass. He was currently receiving outpatient treatment for TB with a four-drug regimen (RIPE therapy: rifampin, isoniazid, pyrazinamide, and ethambutol) coordinated by infectious disease specialists and the Department of Health. On initial evaluation, the patient was hemodynamically stable (normal vital signs) with mild tenderness in his right lower abdomen. Laboratory tests revealed a mild elevation in white blood cell count.
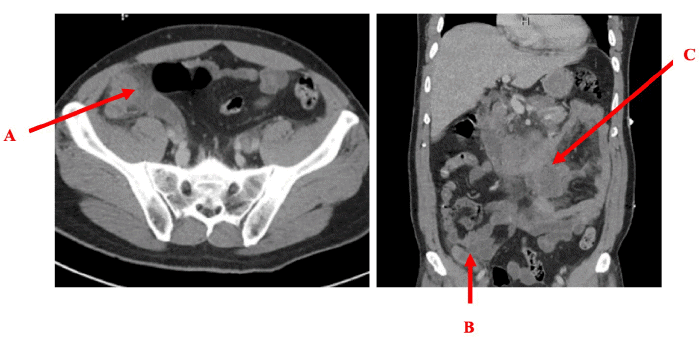
The patient underwent abdominal and pelvic CT imaging, which was significant for a moderately-sized peripherally-enhancing conglomerate of central mesenteric lymph nodes in the left central mesentery, with concerning invasion into the third portion of the duodenum (Figure 1). Additionally, the CT scan showed an enlarged appendix with surrounding peri-appendiceal stranding and a lobulated soft tissue mass in the right paracolic gutter connected to the tip of the appendix. These findings were all suggestive of potential TB involvement.
Figure 1. Abdominal CT Scan. Published with Permission
He was admitted with a multidisciplinary approach involving infectious disease, pulmonology, gastroenterology, and surgery. RIPE therapy was continued, and his appendicitis was managed nonoperatively with a 10-day course of piperacillin/tazobactam antibiotics.
The patient's clinical course was complicated by conflicting findings on repeat CT imaging performed on hospital day 3. While there was radiographic improvement of known tuberculosis lesions within the chest and abdomen, a concerning progression of lymphadenopathy was identified. This included enlargement of lymph nodes in the right hilar region, mediastinum, left supraclavicular/lower cervical chain, right axilla, and paratracheal space, with concerning evidence of invasion into the superior vena cava (SVC). The appendix appeared stable on the repeat CT scan.
Given the discordant findings of improving tuberculosis lesions yet worsening lymphadenopathy, a neoplastic process became a significant concern. This prompted a right axillary lymph node biopsy, which ultimately revealed poorly differentiated carcinoma of unknown primary origin on pathology analysis.
Further workup to identify the primary tumor site was planned, with endobronchial ultrasound scheduled to investigate the possibility of a lung primary, but the patient made the decision to leave the hospital against medical advice on hospital day 7.
He was readmitted less than one month later after an outpatient brain MRI for headache revealed new intracranial TB lesions. In the interim, he experienced poor oral intake secondary to abdominal pain and vomiting. Surgical consultation was obtained for gastric outlet obstruction and recurrent appendicitis.
While the patient was continued on RIPE therapy with dexamethasone and piperacillin/tazobactam, the surgical approach was palliative, focusing on relieving his gastric outlet obstruction. The proposed procedures included a gastrojejunostomy bypass to create a new passage for food to bypass the obstruction, a gastrostomy tube for feeding support, and an appendectomy to address the recurrent appendicitis.
Following extensive discussions involving a multidisciplinary team, the patient opted for a non-surgical approach, prioritizing traditional healing methods. He eventually consented to several rounds of palliative abdominal and mediastinal radiation therapy. Unfortunately, on hospital day 23, he suffered an aspiration event requiring emergent intubation. This was followed by rapid clinical deterioration and pulseless cardiac arrest. Despite resuscitation efforts, spontaneous circulation could not be re-established.
Discussion
Tuberculosis, caused by the bacteria Mycobacterium tuberculosis, is a life-threatening infection that remains rare in modern Western medicine. According to the CDC, there were 7,171 reported cases of TB nationwide in 2020, resulting in approximately 600 deaths.1 Abdominal TB is a rare complication, affecting 5-10% of patients with TB and arising from hematogenous spread of the bacteria from the lungs. Reactivation of previously dormant pulmonary TB can occur in immunocompromised individuals (e.g., those with HIV, diabetes, renal failure, or malignancy). Ileocecal involvement is present in approximately 75% of abdominal TB cases. Gross pathology demonstrates transverse ulcerations, fibrosis, mesenteric lymph node invasion, and omental thickening.2
In the United States, case reports of abdominal TB are infrequent and diverse in presentation. Three cases were reported as recently as 2021: one identified during a routine colonoscopy,3 another occurring in an immunosuppressed patient following a kidney transplant,4 and a third diagnosed in a patient with decompensated alcoholic cirrhosis.5 Appendicitis secondary to abdominal TB is even rarer, with no published cases in the US since 1994.6 Prior studies have categorized three types of appendiceal involvement in abdominal TB:
- Chronic Ileocecal Disease with Appendiceal Involvement: Approximately 50% of historical cases fall into this category, presenting with intermittent episodes of moderate abdominal pain, nausea, and vomiting over a period of months.7,8
- Acute Obstructive Appendicitis: This presentation mimics typical uncomplicated acute appendicitis.
- Incidental Disease: In some cases, appendiceal TB is only identified on pathology after surgical removal.7,8
Abdominal TB can radiographically resemble ovarian carcinomatosis, lymphoma, and inflammatory bowel disease.9
A recent study from Southeast Asia, where TB remains endemic, found TB appendicitis to be exceedingly rare (0.08% of appendectomies and 0.2% of TB patients).10 Among the five patients identified over a 15-year period, all underwent surgical intervention (laparoscopic or open appendectomy), with only one developing a postoperative complication (surgical site infection and fistula formation).10 These findings suggest that surgical appendectomy can be a safe and reasonable option for many patients with suspected appendicitis, even if TB is ultimately diagnosed postoperatively on pathology. However, for patients with a confirmed diagnosis of abdominal tuberculosis and a suspected case of TB appendicitis, as presented in this case report, medical management is generally preferred. Surgery is typically reserved for recurrent cases or for achieving source control in patients with hemodynamic instability.
Conclusion
This case presents a patient with abdominal tuberculosis causing recurrent appendicitis in the setting of an unknown primary malignancy. Various social determinants of health, both globally and locally, significantly impacted the patient's course. This case highlights the importance of TB screening and treatment in endemic areas and for those who emigrate, emphasizing the role of primary care and public health initiatives. Effective communication within a multidisciplinary healthcare team and with government agencies is crucial for coordinating inpatient and outpatient care. Furthermore, proficiency in utilizing translation services and practicing cultural humility are essential for engaging diverse populations and providing optimal care. This case is ultimately frustrating, as earlier and more complete patient engagement may have prevented premature mortality.
Lessons Learned
Abdominal and appendiceal tuberculosis are rare manifestations of TB, more commonly encountered in specific endemic regions. Medical management of TB and appendicitis is the first-line treatment. Surgical intervention is effective and indicated for recurrent or medically refractory cases. A multidisciplinary approach is crucial when abdominal TB is suspected.
Authors
Mouradian GP; Eaton S
Author Affiliation
Department of Surgery, University of Kansas Medical Center, Kansas City, KS 66160
Corresponding Author
Gregory P. Mouradian, MD
Department of Surgery
University of Kansas Medical Center
3901 Rainbow Boulevard
Mail Stop 2005
Kansas City, KS 66160
Email: gmouradian@kumc.edu
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding/Support
The authors have no relevant financial relationships or in-kind support to disclose.
Received: March 2, 2023
Revision received: April 10, 2023
Accepted: June 27, 2023
References
- Centers for Disease Control and Prevention (CDC). (2022). Table 1. Reported Tuberculosis Cases by State and Territory, 2020 [Data table]. Retrieved from https://www.cdc.gov/tb/statistics/default.htm
- Hassan I, Brilakis ES, Thompson RL, Que FG. Surgical management of abdominal tuberculosis. J Gastrointest Surg. 2002;6(6):862-867. doi:10.1016/s1091-255x(02)00063-x
- Obeidat AE, Namiki T, Murakami TT. More Than Just a Polyp: Diagnosis of Tuberculosis From a Screening Colonoscopy. Cureus. 2021;13(2):e13216. Published 2021 Feb 8. doi:10.7759/cureus.13216
- Jiang JY, Greenwald H, Gupta V. Intestinal Tuberculosis Presenting as an Ileocecal Mass in a Renal Transplant Patient. Cureus. 2021;13(1):e12995. Published 2021 Jan 29. doi:10.7759/cureus.12995
- Park H, Kansara T, Victoria AM, Boma N, Hong J. Intestinal Tuberculosis: A Diagnostic Challenge. Cureus. 2021;13(2):e13058. Published 2021 Feb 1. doi:10.7759/cureus.13058
- Dezfuli M, Oo MM, Jones BE, Barnes PF. Tuberculosis mimicking acute appendicitis in patients with human immunodeficiency virus infection. Clin Infect Dis. 1994;18(4):650-651.
- Ahmed ME, Hassan MA. Abdominal tuberculosis. Ann R Coll Surg Engl. 1994;76(2):75-79.
- Singh MK, Arunabh, Kapoor VK. Tuberculosis of the appendix--a report of 17 cases and a suggested aetiopathological classification. Postgrad Med J. 1987;63(744):855-857. doi:10.1136/pgmj.63.744.855
- Faulhaber S, Schindera S, Hartel M, Gräfitsch A. Report of two rare manifestations of abdominal tuberculosis mimicking neoplasia. J Surg Case Rep. 2022;2022(3):rjac079. Published 2022 Mar 30. doi:10.1093/jscr/rjac079
- Chong VH, Telisinghe PU, Yapp SK, Chong CF. Tuberculous appendix: a review of clinical presentations and outcomes. Singapore Med J. 2011;52(2):90-93.