Abstract
Background
A 30-year-old male with a remote history of trauma presented with a tension gastrothorax. After conservative management measures failed, the patient required an emergent resuscitative thoracotomy to achieve decompression.
Summary
Diaphragmatic injuries are frequently encountered, usually secondary to thoracoabdominal trauma. In some patients, these injuries can lead to the formation of a diaphragmatic hernia. While often asymptomatic, diaphragmatic hernias can cause life-threatening complications, most notably, tension gastrothorax.
Conclusion
Prompt recognition of tension gastrothorax is critical, as patients can deteriorate rapidly due to the development of tension physiology. The clinical presentations of tension pneumothorax and tension gastrothorax share considerable overlap, making accurate differentiation critical for timely and appropriate intervention.
Key Words
thoracic surgery; tension gastrothorax; diaphragmatic hernia
Case Description
Diaphragmatic injuries are a relatively common occurrence secondary to blunt and/or penetrating thoracoabdominal trauma, with an estimated prevalence of between 1.1% to 3.9%.1 The sequelae of these injuries is the formation of a diaphragmatic hernia. Tension gastrothorax, a unique life-threatening complication, occurs when a progressively dilating stomach herniates into the chest, causing mediastinal shift and tension physiology.2 Tension gastrothorax is rarely documented secondary to a distant traumatic event.3
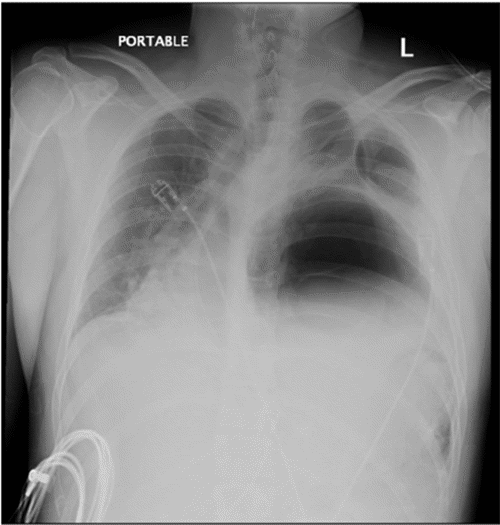
Our patient is a 30-year-old male with a remote history of a severe motor vehicle collision nine years prior, who presented to an outside hospital with several days of worsening abdominal pain and vomiting. A chest X-ray raised concern for a diaphragmatic hernia, leading to placement of a nasogastric tube at the outside hospital. Follow-up X-ray after placement with nasogastric suctioning showed no improvement (Figure 1). His condition continued to decompensate while awaiting transfer to our high-volume teaching hospital, ultimately requiring intubation and vasopressor support for hemodynamic instability.
Figure 1. Persistent Rightward Mediastinal Shift in Tension Gastrothorax. Published with Permission
Upon arrival at our emergency department, the patient was in critical condition and quickly went into cardiac arrest. Advanced cardiac life support (ACLS) protocols were initiated, successfully restoring his vital signs. Given the urgency of the situation, the decision was made to perform an emergency resuscitative thoracotomy in the emergency department.
During the thoracotomy, multiple loops of ischemic and gangrenous colon were visualized within the chest cavity (Figure 2). These were emergently removed. The stomach was found to be massively dilated, filling the entire hemithorax and preventing reduction. A small gastrotomy was performed, and a Foley catheter inserted to decompress the stomach. This intervention successfully relieved tension and led to immediate improvement in the patient’s hemodynamics. He was then stabilized and transferred to the operating room for definitive surgical repair.
Figure 2. Ischemic Colon in Tension Gastrothorax. Published with Permission
In the operating room, a diaphragmatic defect was identified through both a thoracotomy and a midline laparotomy incision. The abdominal contents were successfully reduced back into the abdominal cavity. The diaphragmatic defect had sufficient laxity to allow for primary closure in two layers without requiring mesh reinforcement. The general surgery team then proceeded with a subtotal colectomy and end ileostomy due to the extensive colonic involvement, with gangrene extending from the proximal transverse colon to the proximal sigmoid colon. An upper endoscopy revealed viable gastric mucosa, allowing for a primary closure of the gastrotomy.
The postoperative course was complicated. On postoperative day 11, a CT scan revealed pneumoperitoneum, leading to the discovery of a large perforation at the level of the pylorus. The general surgery team subsequently performed a subtotal gastrectomy with gastrojejunal reconstruction to address this issue. His course was further complicated by intra-abdominal abscesses, a duodenal stump leak, and an anastomotic leak requiring drainage and repair, as well as an episode of pancreatitis and a right hepatic lobe infarction, all of which were managed conservatively.
Six months after his initial presentation, the patient underwent a successful planned re-exploration. This surgery addressed the remaining complications, including repair of the duodenal stump, revision of the gastrojejunostomy, and creation of an ileocolonic anastomosis to restore his gastrointestinal continuity. He recovered well from this procedure and was discharged home, tolerating a diet without requiring supplemental total parenteral nutrition.
Discussion
Tension gastrothorax, a rare but life-threatening complication of diaphragmatic hernia, traditionally relies on nasogastric tube placement for decompression, sometimes accompanied by chest tube insertion.4,5 This case report describes, to our knowledge, the first successful management of tension gastrothorax using a resuscitative thoracotomy performed in the emergency department setting.
Prompt diagnosis is critical, as patients with tension gastrothorax can deteriorate rapidly due to the swift development of tension physiology. Several etiologies, including cardiac tamponade, pneumothorax, hydrothorax, and gastrothorax, can present with overlapping symptoms. While the clinical presentation of tension pneumothorax and tension gastrothorax share similarities, careful examination of chest X-rays with a high index of suspicion can aid in differentiation. Patients with tension pneumothorax typically experience improvement following chest tube placement, whereas those with tension gastrothorax require decompression of the stomach via a nasogastric tube.6 However, as demonstrated in our case, this may not always be successful.
Diaphragmatic hernias are typically repaired transabdominally. However, in acute settings where intrathoracic contents become massively distended and cause tension physiology, thoracotomy becomes the only viable option. For critically ill patients who fail to improve with nasogastric tube placement and continue to decompensate, a thoracotomy offers the only means to alleviate intrathoracic pressure by manually reducing the herniated contents. This case highlights the importance for surgeons to recognize and utilize thoracotomy as a potentially lifesaving intervention in similar situations.
Conclusion
Tension gastrothorax is a life-threatening complication that can arise from diaphragmatic hernias. Prompt intervention is critical to alleviate the tension physiology and prevent devastating consequences. If conservative measures fail to achieve decompression, surgical intervention becomes necessary and may need to be performed outside of a traditional operating room setting.
Lessons Learned
Acute diaphragmatic hernias require aggressive management strategies. Incarcerated abdominal viscera can rapidly lead to tension physiology, highlighting the urgency of intervention. However, delays may occur in accessing a fully equipped operating room. Therefore, all available options for decompressing the massively distended viscera should be considered. While nasogastric tube drainage is the initial approach, it is crucial to recognize its potential limitations in resolving tension caused by an incarcerated diaphragmatic hernia. If conservative measures prove unsuccessful, there should be no hesitation to proceed with emergent thoracotomy, even within the emergency department setting, to achieve definitive decompression.
Authors
Lee DDa; Renz Cb; Greenstein Ab; Hiotis Sb; Iyer Kc
Author Affiliations
- Department of Thoracic Surgery, Icahn School of Medicine at Mount Sinai, New York, NY 10029
- Department of Surgery, Icahn School of Medicine at Mount Sinai, New York, NY 10029
- Recanati/Miller Transplantation Institute, Icahn School of Medicine at Mount Sinai, New York, NY 10029
Corresponding Author
Dong-Seok Daniel Lee, MD
Department of Thoracic Surgery
Icahn School of Medicine at Mount Sinai
Thoracic Surgery, Mount Sinai Queens
1 Gustave L. Levy Place, Box 1023
New York, NY 10029
Email: dong-seok.lee@mountsinai.org
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding/Support
The authors have no relevant financial relationships or in-kind support to disclose.
Received: April 11, 2023
Revision received: June 22, 2023
Accepted: June 27, 2023
References
- Rubikas R. Diaphragmatic injuries. Eur J Cardiothorac Surg. 2001;20(1):53-57. doi:10.1016/s1010-7940(01)00753-9
- Ordog GJ, Wasserberger J, Balasubramaniam S. Tension gastrothorax complicating post-traumatic rupture of the diaphragm. Am J Emerg Med. 1984;2(3):219-221. doi:10.1016/0735-6757(84)90008-1
- Horst M, Sacher P, Molz G, Willi UV, Meuli M. Tension gastrothorax. J Pediatr Surg. 2005;40(9):1500-1504. doi:10.1016/j.jpedsurg.2005.05.079
- Slater RG. Tension gastrothorax complicating acute traumatic diaphragmatic rupture. J Emerg Med. 1992;10(1):25-30. doi:10.1016/0736-4679(92)90006-f
- Phelan J, Subramanian R, Menon AKK. Acute atraumatic peri-arrest tension gastrothorax presenting to the emergency department. BMJ Case Rep. 2021;14(4):e240478. Published 2021 Apr 8. doi:10.1136/bcr-2020-240478
- Miyahara M, Kondo N, Sugiyama T, Matsumura Y. Resuscitation from Cardiac Arrest with Tension Gastrothorax Due to Acquired Diaphragmatic Hernia. Am J Emerg Med. 2022;60:229.e1-229.e3. doi:10.1016/j.ajem.2022.07.054