Abstract
Background
Gallbladder injury is rare due to its protected position, embedded in the liver and covered by the rib cage. It occurs in 1-2% of blunt trauma injuries and usually accompanies injury to the liver and other organs. A literature review in 1981 found only 101 cases of traumatic injury (many of them contusions), with individual case reports comprising the majority. Isolated gallbladder injury from blunt trauma occurs in just 2% of all gallbladder injuries. Vague symptoms and signs and inconclusive imaging findings make diagnosis challenging, and diagnosis is often made at laparotomy. Morbidity and mortality are usually due to associated injuries but can occur even in isolated injuries.
Summary
We present a rare case of isolated gallbladder perforation in a 34-year-old male with a history of alcohol abuse, who presented with vague abdominal pain and distension. Initially, the patient did not disclose a history of trauma. However, initial CT and ultrasound scans revealed ascites, indicative of alcohol abuse-related cirrhosis rather than gallbladder issues. Further investigation through ultrasound-guided paracentesis revealed bilious fluid, raising suspicion of gallbladder or bile duct involvement. A small bowel series showed no abnormalities, but a HIDA scan detected bile leakage around the gallbladder, suggesting rupture. Subsequent diagnostic laparoscopy confirmed a 3 cm laceration in the gallbladder infundibulum with no other organ injuries noted. Laparoscopic cholecystectomy was then successfully performed, and the patient was discharged in stable condition.
During a follow-up clinic visit, the patient complained of right-sided chest pain. A CT chest scan revealed previously undetected fractures of right-sided ribs 5 and 6, consistent with blunt trauma. Upon further questioning post-surgery, the patient admitted to a “fall” resulting in right chest injury but provided limited details. Nonetheless, the patient’s recovery progressed uneventfully.
Conclusion
Diagnosing isolated traumatic rupture of the gallbladder preoperatively is challenging, and it is typically identified during laparotomy. Symptoms and signs are relatively mild, and when the patient does not volunteer a history of trauma, even imaging can be inconclusive. A history of alcohol abuse is a common scenario. This case underscores the importance of a thorough history and physical examination with focused diagnostic imaging when faced with bilious ascites. The gallbladder is generally soft and without calculi or inflammatory change. In this case, an extensive but expeditious work-up allowed for the completion of laparoscopic cholecystectomy and a good outcome.
Key Words
gallbladder perforation; traumatic rupture; bilious ascites; hepatobiliary; trauma; acute abdomen
Case Description
A 34-year-old male with anxiety disorder, depression, alcohol and opioid substance abuse disorder, and Wolff-Parkinson-White syndrome status post ablation presented to the emergency room complaining of worsening generalized abdominal discomfort. The pain was described as sharp, with a severity rating of 6 out of 10, and it radiated to the back. It began four weeks ago during a hospitalization at an outside facility due to loss of consciousness from events that he could not recall. His last alcohol intake was two days prior to admission. Vital signs were normal. On examination, he had mild diffuse abdominal tenderness without guarding. Admission laboratory studies (Table 1) were notable for leukocytosis with neutrophilic predominance and mild transaminitis.
Abdominal ultrasound on admission showed ascites without evidence of acute cholecystitis. The patient was admitted to the medical service initially and empirically given antibiotics. A non-contrast computed tomography (CT) scan confirmed ascites and a “contracted gallbladder.” Interventional radiology performed an ultrasound-guided paracentesis via right lower quadrant entry, which was noted to be atraumatic and yielded 1100 mL of dark-amber-colored fluid. A fluid analysis demonstrated elevated bilirubin to 15.5 mg/dL. Differential diagnoses included small bowel perforation, perforated peptic ulcer, and injury to the biliary tree.
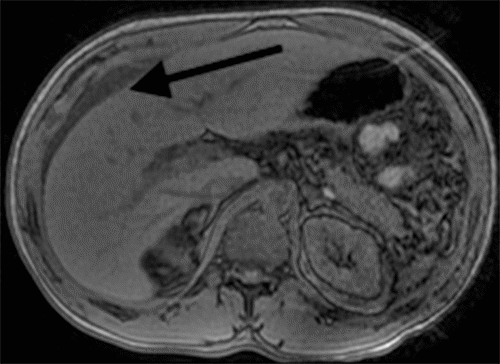
While the patient reported initial relief of symptoms within 48 hours of the initial procedure, he experienced a recurrence of nausea, distension, and abdominal pain. Post paracentesis, CT imaging of the abdomen pelvis failed to show extravasation of oral contrast from viscera (Figure 1) but revealed a contracted gallbladder and re-accumulation of ascites. A hepatobiliary iminodiacetic acid (HIDA) scan showed a biliary leak from the region of the gallbladder fossa (Figure 2). Magnetic resonance cholangiopancreatography showed recurrent ascites but no biliary obstruction (Figure 3). No traumatic injuries were identified on the initial imaging. Repeat paracentesis yielded one liter of bilious fluid, again with a resolution of symptoms.
Figure 1. CT Abdomen and Pelvis with Oral and Intravenous Contrast Showing Ascites and Contracted Gallbladder (arrows). Published with Permission
The patient was taken for diagnostic laparoscopy, which revealed a 3 cm perforation of the gallbladder at the level of the infundibulum along the cystic plate with biliary peritonitis (Figure 4). Abdominal washout was undertaken with copious irrigation, and a laparoscopic cholecystectomy was completed without complication. The postoperative course was uneventful, and the patient was discharged two days later.
At his postoperative visit a week later, he complained of persistent abdominal and chest wall pain, prompting repeat imaging, which revealed no intraabdominal abnormalities. However, fractures of the right fifth and sixth ribs of indeterminate age were noted, consistent with trauma (Figure 5). On further questioning, the patient admitted to a fall several weeks prior with trauma to his right chest and reiterated he did not recall the events leading to his initial hospitalization at the outside facility. The pain had resolved by the time of his follow-up visit two weeks later. Pathology confirmed gallbladder perforation without cholelithiasis or inflammation.
Discussion
Gallbladder perforation, in general, is rare, with an incidence rate of 2-11%.1 It often represents a complication of acute calculous cholecystitis or iatrogenic injury during cholecystectomy.2 While the earliest documentation of gallbladder perforation was in 1844, Niemeier published the first classification system in 1934.3 Type I represents perforations with free intraperitoneal bile leak. While less common than contained perforations with abscess (Type II), they represent a significant risk for morbidity and mortality, often presenting with signs of sepsis and peritonitis.4,5 Type I perforations may present as a surgical emergency requiring urgent operative intervention to obtain source control.6 Common findings in patients with perforation include increased leukocytosis, elevated c-reactive protein levels, older age, and male gender. Predisposing risk factors include severe infection, malignancy, trauma, pharmaceuticals such as steroids, diabetes, and coronary artery disease. Non-traumatic perforations are seen at the level of the fundus, mainly secondary to ischemia.2,7,8
Gallbladder perforation from blunt trauma is rarer and is usually associated with injuries to other organs, especially the liver. Isolated gallbladder injuries are extremely rare, can have delayed presentation, and represent just 1-2% of gallbladder injuries.9,10,11 They pose a diagnostic challenge because of vague signs, symptoms, and inconclusive imaging, as was seen here. The sterile nature of traumatic rupture is thought to lead to chemical peritonitis rather than infectious. Conventional findings in clinical presentation and laboratory values seen in “classic” biliary peritonitis are often absent, including toxemia, shock, hyperbilirubinemia, and transaminitis. In fact, patients returning days or weeks after discharge from their initial traumatic accident with indistinct symptoms of generalized abdominal pain are often reported in the literature.9,11
While ultrasound remains the diagnostic imaging modality of choice in acute biliary pathology, it has a reported sensitivity of only 58% for detecting perforation. On the other hand, HIDA scans demonstrate superior sensitivity (89%) in detecting free gallbladder perforation. Although CT scans may aid in identifying ascites in Type I perforations, distinguishing bilious ascites from simple ascites based solely on Hounsfield units is not possible.6,7 The use of magnetic resonance imaging (MRI) has been documented in the literature, primarily due to its ability to detect mural discontinuity in the gallbladder wall and stones within the biliary tree and dilatation.1,2,13 This clarity in imaging often aids in surgical planning by delineating the need for intervention at the level of the biliary tree versus solely the gallbladder.
In a patient with undifferentiated abdominal pain and distension, the initial identification of ascites occurs most often via abdominal ultrasound or CT imaging. Decision-making for further imaging and treatment is based on presumed type and etiology. Without anchoring history or physical exam findings, paracentesis is generally the next step in care, as it provides fluid for analysis and diagnosis. While iatrogenic injury must always be considered when encountering bilious ascites, the timing of symptoms with respect to the procedure and fluid analysis is critical. In this case, the patient had documented symptoms and moderate volume ascites prior to paracentesis, and fluid analysis revealed a 14:1 ratio of ascites to serum bilirubin. Given this, along with the use of image-guided atraumatic technique, it is unlikely that iatrogenic injury contributed to this patient’s pathology. Additional imaging, including CT, HIDA, and MRCP, was completed in this case due to concerns for acute change in clinical status as well as the need to confirm biliary rupture and the desire to identify the location of disruption. It should be noted that a confirmed biliary leak on HIDA scan represents sufficient evidence necessitating operative intervention. Following the diagnosis of bilious ascites, both HIDA and MRCP are individually reasonable options for imaging to localize the site of perforation; however, utilization of both modalities is not commonly employed.
Perforation following blunt trauma is more common in patients with thin-walled, distended gallbladders and recent ingestion of alcohol.12,13 While motor vehicle injuries and falls may cause gallbladder perforations alongside other organ injuries, isolated gallbladder rupture appears to be mostly associated with localized forceful blows and sports injuries.10 Isolated injuries range from contusions to ruptures and avulsions (traumatic cholecystectomy).10,12,13 Associated injuries often lead to morbidity and mortality. Previously, management options included cholecystostomy and gallbladder repair. The current consensus favors cholecystectomy, preferably laparoscopic, whenever feasible.1,2,4,7 In this patient’s case, we postulate a mechanism involving traumatic avulsion of the infundibulum after a forceful blow via crush injury during his fall. Given the location on the posterior portion of the infundibulum where the peritoneal attachments to the liver begin, iatrogenic injury during paracentesis is exceedingly unlikely.
Even though the first documentation of gallbladder perforation was published in the early 20th century, understanding this clinical entity remains limited. Individual case reports comprise the majority of data currently available in the literature. Aggregate analysis of these reports allows for inference regarding the etiology, incidence, and outcomes of free rupture in order to guide diagnosis and management.
Conclusion
Gallbladder rupture may occur due to minor, unreported trauma and can manifest subtly, particularly among individuals who abuse alcohol. Thorough history-taking and diligent investigation are vital in arriving at a diagnosis before surgery. If a patient with abdominal pain and otherwise unrevealing clinical history and examination is found to have ascites on ultrasound or CT imaging, we recommend diagnostic paracentesis. Should bilious ascites be identified, further imaging with a HIDA scan or MRCP can be pursued to identify and document the biliary leak. Therapeutic intervention will be dictated by the location of rupture and the presence of stones. In those cases of isolated gallbladder rupture, laparoscopic cholecystectomy is the optimal treatment. Management of perforation associated with trauma versus malignancy is dramatically different, and misdiagnosis may significantly affect outcomes.
Lessons Learned
Ascites and abdominal pain in individuals who abuse alcohol may not always be attributed to cirrhosis. Paracentesis is useful and can start the diagnostic cascade to define rarities like an isolated rupture. HIDA scans are often the best tool for diagnosis. Early operative intervention for Type I perforations directly affects morbidity and mortality.
Authors
Lotakis DM; Chung MY; Wallack MK; Mariadason J
Author Affiliations
Department of Surgery, NYC Health + Hospitals/Metropolitan, New York, NY 10029
Corresponding Author
Dimitra Maria Lotakis, MD
Metropolitan Hospital Center-Surgery
1901 1st Avenue
Bronx, NY 10471
Email: dlotakis@gmail.com
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding/Support
The authors have no relevant financial relationships or in-kind support to disclose.
Received: April 26, 2021
Revision received: July 18, 2021
Accepted: July 27, 2021
References
- Sahbaz NA, Peker KD, Kabuli HA, Gumusoglu AY, Alis H. Single center experience in laparoscopic treatment of gallbladder perforation. Wideochir Inne Tech Maloinwazyjne. 2017;12(4):372-377. doi:10.5114/wiitm.2017.72321
- Gunasekaran G, Naik D, Gupta A, et al. Gallbladder perforation: a single center experience of 32 cases. Korean J Hepatobiliary Pancreat Surg. 2015;19(1):6-10. doi:10.14701/kjhbps.2015.19.1.6
- Niemeier OW. Acute Free Perforation of the Gallbladder. Ann Surg. 1934;99(6):922-924. doi:10.1097/00000658-193499060-00005
- Date RS, Thrumurthy SG, Whiteside S, et al. Gallbladder perforation: case series and systematic review. Int J Surg. 2012;10(2):63-68. doi:10.1016/j.ijsu.2011.12.004
- Pavlidis TE, Lalountas MA, Psarras K, et al. Isolated complete avulsion of the gallbladder (near traumatic cholecystectomy): a case report and review of the literature. J Med Case Rep. 2011;5:392. Published 2011 Aug 18. doi:10.1186/1752-1947-5-392
- Jansen S, Stodolski M, Zirngibl H, Gödde D, Ambe PC. Advanced gallbladder inflammation is a risk factor for gallbladder perforation in patients with acute cholecystitis. World J Emerg Surg. 2018;13:9. Published 2018 Feb 20. doi:10.1186/s13017-018-0169-2
- Derici H, Kara C, Bozdag AD, Nazli O, Tansug T, Akca E. Diagnosis and treatment of gallbladder perforation. World J Gastroenterol. 2006;12(48):7832-7836. doi:10.3748/wjg.v12.i48.7832
- Swayne LC, Filippone A. Gallbladder perforation: correlation of cholescintigraphic and sonographic findings with the Niemeier classification. J Nucl Med. 1990;31(12):1915-1920.
- D’Souza C, Bhagavan KR, Rakesh K. Isolated gall bladder perforation following a blunt injury in the abdomen. J Clin Diagn Res. 2012;6(8):1409-1410. doi:10.7860/JCDR/2012/4034.2371
- Bainbridge J, Shaaban H, Kenefick N, Armstrong CP. Delayed presentation of an isolated gallbladder rupture following blunt abdominal trauma: a case report. J Med Case Rep. 2007;1:52. Published 2007 Jul 16. doi:10.1186/1752-1947-1-52
- Soderstrom CA, Maekawa K, DuPriest RW Jr, Cowley RA. Gallbladder injuries resulting from blunt abdominal trauma: an experience and review. Ann Surg. 1981;193(1):60-66. doi:10.1097/00000658-198101000-00010
- Schachter P, Czerniak A, Shemesh E, Avigad I, Lotan G, Wolfstein I. Isolated gallbladder rupture due to blunt abdominal trauma. HPB Surg. 1989;1(4):359-362. doi:10.1155/1989/95937
- Birn J, Jung M, Dearing M. Isolated gallbladder injury in a case of blunt abdominal trauma. J Radiol Case Rep. 2012;6(4):25-30. doi:10.3941/jrcr.v6i4.941