Abstract
Background
A 63-year-old male presented with a symptomatic large left-side diaphragmatic hernia five years following a motor vehicle accident.
Summary
We present an interesting case of a 63-year-old male complaining of severe mid-abdominal pain and progressive dyspnea. He was a pedestrian struck by a motor vehicle five years ago, with no overt trauma noticed at the time. However, he exhibited progressive posttraumatic dyspnea that was attributed to COPD exacerbation. Subsequent studies with chest X ray and abdominopelvic CT scan demonstrated the finding of a grade IV hiatal hernia on the left side. The patient underwent a transabdominal laparoscopic repair of the diaphragmatic hernia with a relaxing incision, primary closure, and absorbable mesh reinforcement. The patient did well postoperatively and had a resolution of his abdominal pain and dyspnea to the point that he ceased requiring home oxygen therapy.
Conclusion
Delayed life-threatening complications can arise following a traumatic car accident. This interesting case sheds light on the importance of careful history-taking and re-evaluation of differential diagnoses when an initial diagnosis may be incorrect.
Key Words
diaphragmatic hernia; dyspnea; COPD; abdominal pain; trauma
Case Description
A 63-year-old male with a past medical history of hypertension, peptic ulcer disease, tobacco use, and aneurysm of ascending aorta presented to the emergency department (ED) complaining of constant severe mid-abdominal pain for several hours and emesis. He denied prior occurrences and had no other symptoms. He had a past surgical history of exploratory laparotomy for a perforated duodenal ulcer 30 years prior. He was a chronic lifelong smoker with a 40-pack year history. Of note, he was involved in a pedestrian struck by a motor vehicle accident five years prior. He was not diagnosed with any significant injuries at the time. However, after the accident, the patient endorsed progressive positional dyspnea, eventually leading to intermittent supplemental home oxygen therapy.
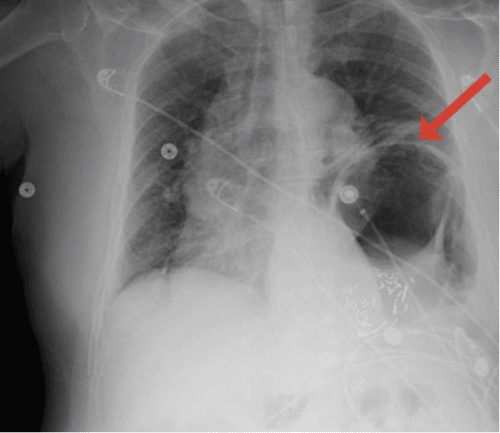
On physical examination, his abdomen was soft, non-distended, and had generalized tenderness with no guarding or rigidity. A bedside ultrasound of the abdomen did not show significant findings. Chest X ray revealed significant elevation of the left hemidiaphragm with a prominent distended gastric bubble within the left thoracic cavity (Figure 1). An abdominopelvic CT demonstrated a type IV traumatic diaphragmatic hernia on the left, which contains the splenic flexure of the colon and most of the stomach (Figure 2).
Figure 1. Chest X Ray Showing Left Diaphragmatic Hernia with Distended Gastric Bubble within Left Thoracic Cavity. Published with Permission
Figure 2. Abdominopelvic CT with Contrast Demonstrating Hiatal Hernia Containing Splenic Flexure and Stomach in A) Sagittal Section and B) Axial Section. Published with Permission
The intrathoracic stomach within the hernia was dilated with air and fluid; however, there was no transition point indicating evidence of obstruction. Nasogastric decompression and fluid resuscitation were implemented, and after careful counseling and consent, the patient was taken to the operating room for planned transabdominal laparoscopic repair of the diaphragmatic hernia. Upon laparoscopic entry into the abdomen, dense adhesions were found in the upper abdomen, consistent with the patient's prior open repair of a perforated gastric ulcer. This made the entire upper abdomen technically difficult to dissect out and identify anatomy. Extensive intraabdominal lysis of adhesions was required to visualize the hernia. The defect measured 9.5 cm transversely and 4.5 cm in the anterior-posterior dimension. Upon reduction of the hernia, the left lung was noted to be severely atelectatic; it expanded eventually with ventilation. A relaxing incision in the diaphragm was made, and the defect closed transversely with several non-absorbable v-lock sutures. The repair was then reinforced with onlay absorbable mesh (Phasix ST) (Figure 3).
Figure 3. Intraoperative Images. Published with Permission
The patient tolerated the procedure well. He remained intubated postoperatively and was transferred to the intensive care unit for recovery. On postoperative day 1, the patient was successfully extubated. An upper GI X ray on postoperative day 3 confirmed an intact repair (Figure 4).
Figure 4. Upper GI X Ray Demonstrating Stomach Projecting Under Diaphragm A) Before and B) After Contrast. Published with Permission
The patient was discharged on postoperative day 7 with aggressive respiratory therapy and pulmonary toilet. The patient was pain-free on follow-up without dyspnea or home oxygen requirements.
Discussion
Traumatic diaphragmatic injury may acutely present with herniation of abdominal viscera into the thoracic cavity; however, there can be a delay in diagnosis, such as in our case. Motor vehicle accidents are estimated to account for 5% of posttraumatic diaphragmatic hernias and injuries relating to the abdominal cavity that are either misdiagnosed or delayed in clinical.1 Symptomatic presentation years after initial trauma can manifest as perforation, incarceration, obstruction, and strangulation, causing ischemia.1 Late presentation for traumatic diaphragmatic hernia has been hypothesized to occur for different reasons. Omentum and viscera from the abdominal cavity can temporarily plug the diaphragmatic defect until actual herniation occurs.2 This can explain how small diaphragmatic hernias may remain asymptomatic.2 Another theory is that radiological images can be incorrectly read and diagnosed initially after trauma.1 In this case, our patient was diagnosed with symptomatic diaphragmatic hernia five years after his accident. Traumatic diaphragmatic hernias can be categorized into the left side, accounting for 69 %, right-sided for 24%, and bilateral for 15%.3
Common gastrointestinal viscera that can herniate into the thoracic cavity include the omentum, stomach, liver, spleen, small intestine, and colon.2 Important symptoms of a diaphragmatic hernia are chest pain, dyspnea, epigastric discomfort, nausea, vomiting, and abdominal pain.4 Bowel sounds can be heard on the side of herniation, with the left side seeing the vast majority of hernias due to relative protection of the right side by the liver.2 An initial chest X ray may demonstrate air-fluid levels and a bowel gas pattern within the thoracic cavity. Other imaging may be required if initial images are unclear, including ultrasound, CT, MRI, and upper GI series.4 Some radiographic signs include the mediastinal shift to the contralateral side, obscuration of the diaphragmatic margin, elevated hemidiaphragm, and bowel shadowing in the thoracic cavity.2 Injuries such as hemothorax, pneumomediastinum, pneumoperitoneum, and lower rib fractures can be associated with diaphragmatic injuries.4 Our patient had worsening dyspnea after his accident to the point that he increasingly relied on home oxygen therapy. Because of poor follow-up to care, he was misdiagnosed with COPD until his last presentation.
Surgery is the treatment of choice for diaphragmatic hernias, with the two major approaches being either transabdominal or transthoracic.5 Either approach can be performed through an open incision or minimally invasively. Acute, unstable trauma patients with diaphragmatic hernias and hemodynamic instability are typically managed transabdominally with laparotomy since injuries to other abdominal viscera must be concomitantly diagnosed and managed.5 There is a slight risk of concomitant intraabdominal injury during laparotomy of about 30%.6 Delayed cases of hernia can be managed with either approach, with considerations including hernia size, prior surgical operations and presence of adhesions, and patient comorbidities.2 The transthoracic approach typically requires a patient to be able to tolerate single lung ventilation and requires a thoracic surgeon. It is an excellent approach for large hernias that extend well into the thoracic cavity and can be difficult to reduce trans-abdominally. In our patient, his prior abdominal surgical history was an important consideration. The possibility that the procedure could not be completed transabdominally was considered, and a thoracic surgeon was available as needed for assistance.
Diaphragmatic repairs typically consist of closure with non-absorbable sutures. Relaxing incisions can help reduce tension on the closure. Large defects are usually reinforced with mesh, either permanent or absorbable.7 Laparoscopic approaches, either transabdominal or transthoracic, have the typical advantages over open surgeries: reduced pain, hospital stay, and recovery, with improved cosmesis. Additionally, there is a decreased risk of incisional hernias since the associated incisions are comparatively smaller.
A unique highlight of this case is the delay in diagnosis of our patient's diaphragmatic hernia years after his accident. Without having his imaging from the time of his trauma, it is unclear if the hernia was present in its current form but not seen or began as a small defect that gradually increased over time. Given the progression of his symptoms prior to presentation, the second possibility is likely.
Conclusion
The pedestrian struck by a motor vehicle scenario is a large blunt force traumatic event that can cause severe injuries such as traumatic diaphragmatic hernia. Delayed traumatic diaphragmatic hernia can masquerade as other symptoms, such as COPD exacerbation. It is important to maintain an index of suspicion at the time of the initial trauma and carefully evaluate symptoms and imaging. Once diagnosed, it can be repaired via minimally invasive, open, transabdominal, or transthoracic approaches.
Lessons Learned
Delayed diaphragmatic hernia due to motor vehicle accidents can masquerade as other symptoms, such as COPD exacerbation. Nonspecific symptoms can be challenging for a definite diagnosis and can be misdiagnosed. It is important to maintain an index of suspicion at the time of the initial trauma and carefully evaluate symptoms and imaging. This will prevent clinicians from misdiagnoses, delaying the patient's medical treatment, and causing life-threatening complications.
Authors
Luvsannyam Ea; Jain MSb; Britt Éb; Mirji ASc; Tiesenga FMd; Jorge JMd
Author Affiliations
- Avalon University School of Medicine, Youngstown, OH 44505
- Saint James School of Medicine, Park Ridge, IL 60068
- Metropolitan University College of Medicine, Waldorf, MD 20602
- Tiesenga Surgical Associates, Elmwood Park, IL 60707
Corresponding Author
Enkhmaa Luvsannyam, MD
Avalon University School of Medicine
212 Churchill Hubbard Road
Youngstown, OH 44505
Email: luvsenkh@isu.edu
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding/Support
The authors have no relevant financial relationships or in-kind support to disclose.
Received: July 18, 2021
Revision received: January 26, 2022
Accepted: February 8, 2022
References
- Ganie FA, Lone H, Lone GN, et al. Delayed presentation of traumatic diaphragmatic hernia: a diagnosis of suspicion with increased morbidity and mortality. Trauma Mon. 2013;18(1):12-16. doi:10.5812/traumamon.7125
- El-Yakub AI, Bello UM, Sheshe AA, Naaya HU. Delayed Presentation of Posttraumatic Diaphragmatic Hernia Masquerading as Recurrent Acute Asthmatic Attack. Case Rep Med. 2017;2017:5037619. doi:10.1155/2017/5037619
- Ahmad Ganie F, Nabi Lone G, Chowdhary M, Lone H. The Characteristics and Surgical Approach in Post-Traumatic Diaphragmatic Hernia: A Single Center Experience. Bull Emerg Trauma. 2013;1(3):108-111.
- Lal S, Kailasia Y, Chouhan S, Gaharwar A, Shrivastava G. Delayed presentation of post traumatic diaphragmatic hernia. J Surg Case Rep. 2011;2011(7):6. Published 2011 Jul 1. doi:10.1093/jscr/2011.7.6
- Hegarty MM, Bryer JV, Angorn IB, Baker LW. Delayed presentation of traumatic diaphragmatic hernia. Ann Surg. 1978;188(2):229-233. doi:10.1097/00000658-197808000-00016
- D'Souza N, Clarke D, Laing G. Prevalence, management and outcome of traumatic diaphragm injuries managed by the Pietermaritzburg Metropolitan Trauma Service. Ann R Coll Surg Engl. 2017;99(5):394-401. doi:10.1308/rcsann.2017.0029
- Kaur R, Prabhakar A, Kochhar S, Dalal U. Blunt traumatic diaphragmatic hernia: Pictorial review of CT signs. Indian J Radiol Imaging. 2015;25(3):226-232. doi:10.4103/0971-3026.161433