Abstract
Background
Spontaneous celiac artery dissection is a rare vascular event with an unclear incidence. Two similarly rare conditions suggested to predispose individuals to celiac artery dissection are median arcuate ligament syndrome (MALS) and connective tissue disorders.
Summary
We present a patient with a fibrillin-1 gene variance of unknown significance who presented with acute abdominal pain. Ultimately, she was found to have median arcuate ligament compression of the celiac artery with concurrent celiac artery dissection. We outline a multimodal and multidisciplinary management approach to this patient, the outcome of which reinforces that while standard first-line treatment for celiac artery dissection is nonoperative management, minimally invasive approaches may eliminate or significantly improve celiac artery compression and stenosis, thereby reducing important modifiable and/or inciting factors.
Conclusion
Minimally invasive median arcuate ligament release is a safe and effective procedure in selected patients with MALS.
Key Words
median arcuate ligament syndrome; spontaneous isolated celiac artery dissection; minimally invasive procedure
Abbreviations
DUS: duplex ultrasound
CTA: computed tomography angiography
CTD: connective tissue disease
MAL: median arcuate ligament
MALS: median arcuate ligament syndrome
SICAD: spontaneous isolated celiac artery dissection
Case Description
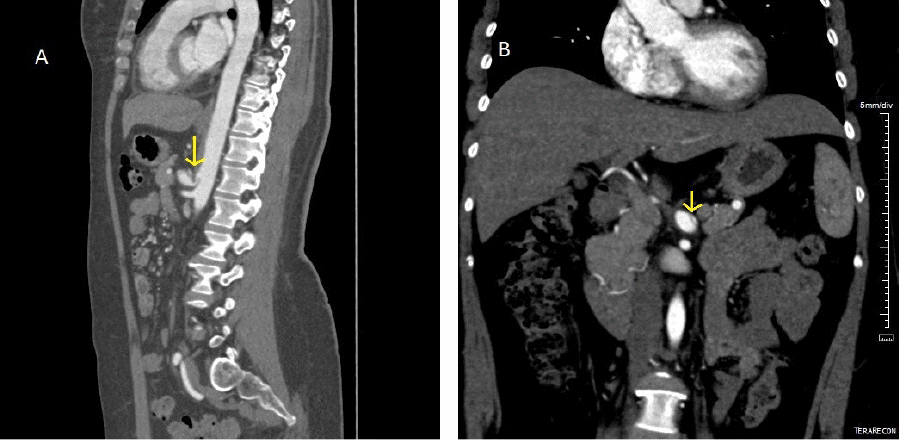
A 46-year-old female nonsmoker presented to the emergency department with acute onset of epigastric pain associated with abdominal bloating and generalized weakness. She noted postprandial pain and nausea while reported having two prior episodes of similar but less intense abdominal pain the preceding week. Her past medical history was notable for anxiety and depression, vasovagal syncope, endometriosis, gastroesophageal reflux disease, chronic constipation, scoliosis, kyphosis, and FBN1 gene variance of unknown significance. Surgical history included multiple operations for endometriosis, transabdominal hysterectomy, and ventral hernia repair. On physical exam, her vitals were normal, and her abdomen was soft, nontender, and nondistended. Right upper quadrant ultrasound demonstrated celiac and proximal splenic artery thrombosis and chronic median arcuate ligament compression of the celiac artery, which was noted to be ectatic. Computed tomography angiography (CTA) showed a 2.9 × 1.3 cm mass near the posterior aspect of the pancreatic body described to be occluding the proximal splenic artery, which raised suspicion for malignancy. Triple-phase enhanced computed tomography (CT) of the abdomen and pelvis demonstrated median arcuate ligament compression with severe celiac artery stenosis (approximately 85%) and post-stenotic dilation, while the posterior pancreatic mass noted on CTA was clarified to be inflammatory thickening of the celiac artery bifurcation (Figure 1A). A dissection of the celiac artery was identified to extend from the poststenotic dilation into the common hepatic artery (Figure 1B). The common hepatic artery was found to be completely occluded with reconstitution of the proper hepatic via collaterals from the gastroduodenal artery. Abdominal Doppler ultrasound (DUS) was performed, confirming median arcuate ligament compression, with celiac axis supine velocities of 455 cm/sec on expiration, 157 cm/sec on inspiration, and 557 cm/sec at rest.
The patient was admitted and started on a heparin nomogram and ondansetron for nausea with pain control as needed. Vascular surgery and gastroenterology consult teams agreed upon nonoperative management. As such, she was counseled by nutrition regarding appropriate diet changes and discharged on apixaban 5 mg by mouth twice daily for three months, with outpatient follow-up with vascular surgery. Her pain subsided while her complete blood count and metabolic panels were within normal limits upon discharge.
Three-month interval CTA abdomen/pelvis re-demonstrated median arcuate ligament compression and post-stenotic celiac artery dilation, with decreased clot burden at the splenic arterial origin (from 2 cm in length on initial imaging to 1 cm) now permitting small passage of contrast. A non-flow limiting dissection of the right renal artery was also noted.
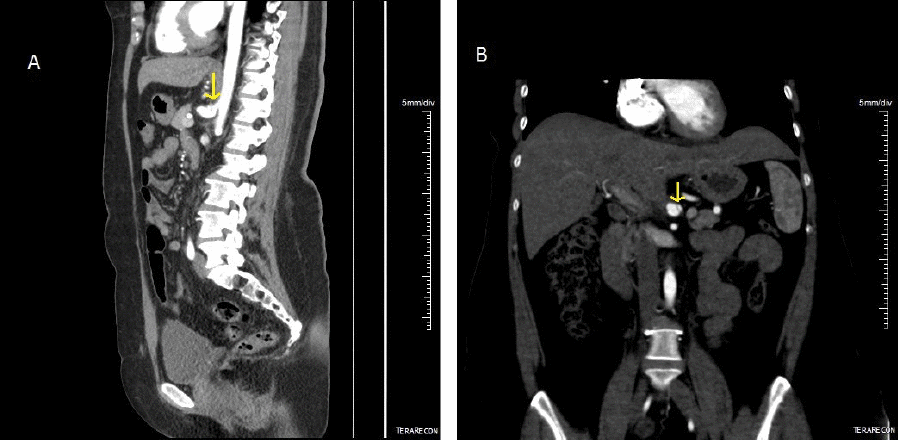
Upon presentation to our institution, the patient reported that her abdominal pain and postprandial pain had largely subsided since starting anticoagulation and making dietary changes. However, she continued to experience some epigastric fullness and discomfort. Mesenteric DUS again demonstrated dynamic elevated velocities consistent with median arcuate ligament compression. She was seen by a minimally invasive surgeon at our institution who specializes in the surgical management of median arcuate ligament syndrome. She underwent further testing per our MALS protocol, including a celiac plexus block by a pain management specialist. She endorsed the temporary resolution of her abdominal symptoms status post-celiac plexus block. Subsequently, she underwent robotic-assisted median arcuate ligament release three months later, which she tolerated well with no recurrence of her symptoms (Figure 2). CTA performed one year later showed stable dissection of the celiac artery and morphology, keeping with her history of MALS (Figure 3). There was no significant change between inspiration and expiration, and the luminal diameter of the proximal celiac artery was significantly improved overall. These findings were consistent with the release of the median arcuate ligament.
Figure 1. Sagittal and Coronal CTA Images. Published with Permission
Figure 2. Robotically Assisted Laparoscopic Release of Median Arcuate Ligament. Published with Permission
Figure 3. One Year Postoperative, Sagittal, and Coronal CTA. Published with Permission
Discussion
Spontaneous isolated celiac artery dissection (SICAD) is a rare phenomenon that occurs without involvement of the aorta but may involve concurrent dissection of other visceral vessels. Although reports of this condition are increasing, owing to improved imaging modalities, SICAD is still uncommon, and the etiology remains unclear.1 Theoretically, the median arcuate ligament may represent a fixed transition point for the origin of SICAD.2 This has led many case reports and series to specify whether a concurrent median arcuate ligament compression was associated with the presented cases of SICAD.3 In one case series of 19 consecutive patients with SICAD, none demonstrated celiac artery compression by MAL on CT.4 In another series, 2 out of 12 patients presenting with SICAD had associated MALS.3 Connective tissue disease has also been reported in association with some cases of SICAD.5,6 We present a unique patient who had radiographic evidence of celiac artery dissection, sonographic evidence of increased arterial flow velocities in the setting of MALS, and an uncommon fibrillin gene variance likely manifesting as a predisposing collagen vascular disorder.
Although most SICAD patients are asymptomatic on presentation and diagnosed incidentally on CTA, patients can present with epigastric pain, mesenteric end-organ malperfusion, and aneurysm formation with or without rupture.7 Patients with MALS typically present with postprandial pain, nausea/vomiting, bloating, unintentional weight loss, and exercise-induced pain.8 Median arcuate ligament compression is present as a normal anatomic variation in a significant proportion of the population; therefore, a celiac plexus block can assist in confirming the diagnosis of MALS.9,10 Celiac plexus blocks are performed with a short-acting local anesthetic with or without corticosteroid injection. The anesthetic effect can last from several hours to days but eventually diminishes. Ablative therapies such as alcohol injection may offer longer-lasting effects (up to several months), which also wane. In theory, additional therapies such as radiofrequency or microwave ablation may obliterate the celiac plexus and provide long-term relief; however, there is an increased risk for vascular injury with these methods secondary to the thermal energy required to create tissue destruction.
For this reason, celiac plexus block is used as a diagnostic, but not therapeutic, measure in the treatment algorithm for MALS. Future research aimed at safe, long-term ablative therapies for the celiac plexus is warranted. At this time, we believe that pain in the setting of MALS is secondary to neurogenic compression of the celiac plexus by the MAL; hypoperfusion is unlikely to be the etiology for pain in these patients.10
Our patient's symptoms were consistent with MALS. She had no mesenteric ischemia, normal lactate levels, or liver function enzymes. Although she did not report unintentional weight loss initially, she admitted a 4 kg weight gain (in three months) after celiac plexus block. Finally, all symptoms resolved after median arcuate ligament release. The diagnosis of MALS is ultimately achieved by a combination of duplex ultrasound, CTA, or MRA and correlating patient symptoms. Ultrasound findings require a peak expiratory velocity of greater than 200 cm/second with dynamic elevated velocities (peak expiratory velocity larger than resting and inspiratory velocities) to entertain a preliminary MALS diagnosis.11 Dynamic changes based on the respiratory cycle are important, as during expiration, the aorta moves cephalically, thus subjecting the celiac artery to further compression by the MAL.
Given her presentation and familial history, this patient underwent prior genetic workup due to high suspicion for a connective tissue disorder. This workup, performed prior to evaluation at our institution, was significant for an FBN1 gene variance of unknown significance (FBN1 c.7999G>A), a genetic abnormality she shares with her son, who possesses pectus excavatum, slight lens subluxation, aortic root dilation, and hypermobile joints. The patient's mother also had a history of aortic aneurysms to 4.9 cm. She was further tested for COL3A1 gene mutations at our institution to rule out milder forms of vascular Ehlers-Danlos syndrome; however, these testing results were negative. Her erythrocyte sedimentation rate and C-reactive protein levels were within normal limits, and there was little suspicion for vasculitis. Overall, the clinical and phenotypic significance of the patient's FBN1 gene variance remains unestablished.
Connective tissue disorders are known risk factors for major arterial dissection, such as of the aorta, carotid, or vertebral artery. Case reports of Ehlers-Danlos syndrome type IV, Marfan syndrome, and fibromuscular dysplasia associated with isolated celiac or superior mesenteric arterial dissections have been published. To our knowledge, there have been no reports of a patient presenting with SICAD in the setting of both MALS and fibrillin-1 gene abnormality. We believe the widespread nature of spontaneous visceral arterial dissection in this patient, which included not only the celiac artery and its immediate branches but also spontaneous dissection of the right renal artery, could be reflective of genetic predisposition to arteriopathy secondary to fibrillin-1 gene variance. Furthermore, the extensive nature of SICAD, in this case, was likely due to synergistic effects of fibrillin gene variance manifesting as a predisposing collagen vascular disorder and MAL compression of the celiac artery, a known risk factor for this pathology.
SICAD can be managed by observation in patients without end-organ malperfusion, with long-term anticoagulation deemed unnecessary for most of the patients.4 Our patient underwent median arcuate ligament release due to the presumptive diagnosis of MALS. Our protocol for surgical management for MALS includes appropriate imaging workup and celiac plexus nerve block to determine whether the physiologic absence of activity by nerve fibers compressed by the median arcuate ligament will result in the resolution of a patient 's pain-related symptoms. Patients who report a positive response to nerve block may then be offered a median arcuate ligament release procedure, most often performed minimally invasively. This patient underwent a robotic-assisted release, an effective approach previously described by our institution.10,12 The patient responded well to treatment, with no recurrence of symptoms, and is being followed every six months by ultrasound for SICAD.
Conclusion
Spontaneous celiac artery dissection is a rare condition that may present with associated dissection and thrombosis of its distal branches. In the absence of visceral ischemia or significant hemorrhage, it is often amenable to nonoperative management alone. Surgeons should consider the role of celiac artery compression by MAL in the propagation of spontaneous dissection.
Lessons Learned
In appropriate cases of MALS, minimally invasive median arcuate ligament release should be offered as it may improve vascular complications and patient symptoms.
Authors
Wilkerson Aa; Sorour AAb; El-Hayek Ka,c,d; Kirksey Lb
Author Affiliations
- Department of General Surgery, Cleveland Clinic, Cleveland, OH 44195
- Department of Vascular Surgery, Cleveland Clinic, Cleveland, OH 44195
- Division of General Surgery, MetroHealth System, Cleveland, OH 44109
- Case Western Reserve University School of Medicine, Cleveland, OH 44106
Corresponding Author
Lee Kirksey, MD
Cleveland Clinic
9500 Euclid Avenue, Desk H32
Cleveland, OH 44195
Email kirksel@ccf.org
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding/Support
The authors have no relevant financial relationships or in-kind support to disclose.
Received: December 9, 2020
Revision received: February 5, 2021
Accepted: March 4, 2021
References
- Sun J, Li DL, Wu ZH, He YY, Zhu QQ, Zhang HK. Morphologic findings and management strategy of spontaneous isolated dissection of the celiac artery. J Vasc Surg. 2016;64(2):389-394. doi:10.1016/j.jvs.2015.12.050
- Dougherty MJ, Troutman DA. Mesenteric arterial dissection. In: Sidawy AN, Perler BA, eds. Rutherford's Vascular Surgery and Endovascular Therapy. 9th ed. Philadelphia: Elsevier; 2019. p. 1771-9.
- Hosaka A, Nemoto M, Miyata T. Outcomes of conservative management of spontaneous celiac artery dissection. J Vasc Surg. 2017;65(3):760-765.e1. doi:10.1016/j.jvs.2016.09.058
- DiMusto PD, Oberdoerster MM, Criado E. Isolated celiac artery dissection. J Vasc Surg. 2015;61(4):972-976. doi:10.1016/j.jvs.2014.10.108
- Sugiura T, Imoto K, Uchida K, et al. Fibromuscular dysplasia associated with simultaneous spontaneous dissection of four peripheral arteries in a 30-year-old man. Ann Vasc Surg. 2011;25(6):. doi:10.1016/j.avsg.2011.02.018
- Nat A, George T, Mak G, Sharma A, Nat A, Lebel R. Celiac artery disease and fatal rupture of a hepatic artery aneurysm in the Ehlers-Danlos syndrome. Proc (Bayl Univ Med Cent). 2014;27(2):116-117. doi:10.1080/08998280.2014.11929077
- Tanaka Y, Yoshimuta T, Kimura K, et al. Clinical characteristics of spontaneous isolated visceral artery dissection. J Vasc Surg. 2018;67(4):1127-1133. doi:10.1016/j.jvs.2017.08.054
- Goodall R, Langridge B, Onida S, Ellis M, Lane T, Davies AH. Median arcuate ligament syndrome. J Vasc Surg. 2020;71(6):2170-2176. doi:10.1016/j.jvs.2019.11.012
- Patel MV, Dalag L, Weiner A, Skelly C, Lorenz J. Inability of conventional imaging findings to predict response to laparoscopic release of the median arcuate ligament in patients with celiac artery compression. J Vasc Surg. 2019;69(2):462-469. doi:10.1016/j.jvs.2018.04.062
- Weber JM, Boules M, Fong K, et al. Median Arcuate Ligament Syndrome Is Not a Vascular Disease. Ann Vasc Surg. 2016;30:22-27. doi:10.1016/j.avsg.2015.07.013
- Brody F, Richards NG. Median arcuate ligament release. J Am Coll Surg. 2014;219(4):e45-e50. doi:10.1016/j.jamcollsurg.2014.07.003
- El-Hayek KM, Titus J, Bui A, Mastracci T, Kroh M. Laparoscopic median arcuate ligament release: are we improving symptoms?. J Am Coll Surg. 2013;216(2):272-279. doi:10.1016/j.jamcollsurg.2012.10.004