Abstract
Background
Intussusception of the appendix is an exceedingly rare pathology with an incidence of 0.01%. It is most commonly found incidentally on imaging or colonoscopy and typically presents in one of four ways: acute appendicitis, vague right lower quadrant abdominal pain, intestinal obstruction, or asymptomatically. Its etiologies are similarly varied and include mucocele, parasite, neuroendocrine tumor, adenocarcinoma, scar nodules, papilloma, and lymphoid hyperplasia; however, endometriosis is a particularly rare cause of appendiceal intussusception. Diagnosis of this condition poses a unique challenge because of its rarity and the variety of diagnostic tools available to surgeons.
Summary
We present a case of a 29-year-old female who presented with several weeks of intermittent epigastric pain and hematochezia with colonoscopy and CT scan concerning for appendiceal intussusception. She underwent a laparoscopic appendectomy and partial cecectomy, where endometriosis was found as the cause of her inverted appendix.
Conclusion
While appendiceal intussusception presents a diagnostic challenge for surgeons, it should be included in the differential for vague right lower quadrant abdominal pain. Proper diagnosis is critical to rule out a malignant cause of intussusception. Surgical intervention is a safe and effective method to diagnose appendiceal intussusception and determine the underlying etiology definitively.
Key Words
appendiceal; appendix; endometriosis; intussusception; laparoscopy; appendiceal carcinoma
Case Description
A 29-year-old female presented with several weeks of epigastric pain and one week of hematochezia. She denied any other symptomatology. She was initially prescribed ondansetron for nausea associated with her pain and omeprazole, which dulled but did not resolve her pain. She reported having a bowel movement every other day and described them as smooth and soft. She had no prior gastrointestinal (GI) evaluation, no previous esophagogastroduodenoscopy (EGD) or colonoscopy, and had never been tested for H. pylori. Family history was negative for inflammatory bowel disease or GI malignancy, including gastric or colon cancer. She reported drinking alcohol three times a week and denied using tobacco and illicit drugs.
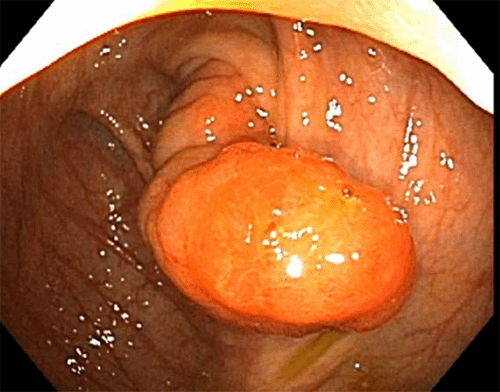
She underwent an EGD and colonoscopy, which was notable for a 30 mm polypoid appearing lesion coming from the appendiceal orifice (Figure 1) and an otherwise normal colon. Biopsies of the lesion showed fragments of colonic mucosa with hyperplastic change, fibrosis, crypt architecture distortion, and focal mild acute and chronic inflammation. A CT showed a tubular structure within the cecum measuring approximately 5 cm in length and 1 cm in width, concerning for an inverted appendix (Figure 2).
Figure 1. Colonoscopy Image of Inverted Appendix. Published with Permission
Figure 2. CT Image Demonstrating Inverted Appendix. Published with Permission
She underwent diagnostic laparoscopy. In the operating room, the appendix and the mesoappendix appeared to be partially intussuscepting into the cecum (Figure 3). It could not be reduced. There were no other abnormalities throughout her abdomen. A laparoscopic appendectomy and partial cecectomy were then performed (Figure 4). The specimen was taken en bloc without needing anastomosis (Figure 5). The frozen section in the operating room was negative for malignancy. Histopathologic evaluation of the specimen revealed an inverted appendix with endometriosis, surface erosion, serrated change, and reactive nuclear atypia. Sections demonstrated endometrial-type glands and stroma involving the appendiceal wall. Positive staining for ER, CK7, and PAX8 supports the diagnosis of an inverted appendix with endometriosis (Figure 6). It was negative for malignancy.
Figure 3. Appendix Partially Intussuscepted Visualized by Laparoscopy. Published with Permission
Figure 4. Schematic of Laparoscopic Appendectomy and Partial Cecectomy.
Figure 5. Gross Specimen of the Appendix and Cecum. Published with Permission
Figure 6. Immunostaining Profile, Demonstrating Endometriosis: A) CK7; B) ER, and C) PAX8. Published with Permission
She was discharged on postoperative day 2 and had a resolution of her pain. The patient was instructed to follow up with her gynecologist. Postoperatively, she recovered well and had full resolution of her initial symptoms at her first follow-up office visit.
Discussion
M'Kidd reported the first case of appendiceal intussusception in 1859 in a seven-year-old boy.1 It is an extremely rare finding and can be caused by a variety of etiologies. The incidence is estimated at 0.01%, according to a cohort study of 71,000 patients over 40 years of age.2,3 Typically, it is found in the first decade of life with a 4:1 male-to-female ratio; however, a growing number of cases are reported in young and middle-aged women.4 The McSwain classification has been proposed to categorize the various types of appendiceal intussusception (Table 1).5
Table 1: The McSwain Classification for Appendiceal Intussusception.6
It often appears as an inverted appendix and typically presents in one of four ways: 1) acute appendicitis with right lower quadrant pain that can be sharp in nature with associated nausea with or without diarrhea or melena, 2) acute obstruction with abdominal distention, nausea, vomiting, 3) vague intermittent abdominal pain with or without melena or anemia, 4) an asymptomatic incidental finding during evaluation for another condition.7‒12 The etiologies vary similarly and include mucoceles, parasites, neuroendocrine tumors, adenocarcinoma, scar nodules, papilloma, and lymphoid hyperplasia.8 The literature suggests a prevalence of appendiceal endometriosis of 0.05%.7,13 Endometriosis of the appendix is a particularly rare cause of appendiceal intussusception, with less than 30 cases in the literature in the last 50 years.14,15 As such, diagnosing an inverted appendix poses a significant diagnostic challenge to physicians.
The vague abdominal pain and hematochezia exhibited in this case made an immediate diagnosis difficult. As such, she underwent a workup involving several modalities, which is common among cases of appendiceal intussusception in the literature.7,8,10‒12,16 Colonoscopy, while invasive, provided direct visualization of the mass and allowed for biopsies to be taken; ultimately, a CT was performed, which was highly suggestive of appendiceal intussusception. CT, ultrasound, and colonoscopy are the most commonly used modalities for modern assessment. However, barium studies were frequently used when such modalities were not readily available and typically showed a cecal filling defect.7,8 Given her persistent abdominal pain and inability to definitively rule out malignancy, she underwent surgical intervention, revealing the nature and etiology of her appendiceal mass. A gross examination of the specimen (Figure 4) identified this case as a type I, based on the McSwain classification.5
There are many reported causes of appendiceal intussusception in the literature. In this case, the biopsies from colonoscopy and surgical specimens were consistent with endometriosis as the cause. Endometriosis of the GI tract has a reported incidence between 5% and 37% and is most commonly found in the sigmoid colon and rectum. Appendiceal endometriosis is even more rare.4,7,11,12,14,15,17 Endometrial deposits are most commonly found in the serosa and muscularis propria, which makes endoscopic diagnosis via biopsy difficult.4 In such cases, hyperplastic and hypertrophic changes and fibrosis and inflammation of the appendix are thought to act as the lead point for intussusception through increased peristaltic movement, which is consistent with biopsies in the present case.4,14,18 Though not found in this case, half of the reported cases of appendiceal intussusception also lead to ileocolic intussusception. Overall, these patients are thought to be more susceptible to intussusception in other parts of the bowel.19
While diagnosing appendiceal intussusception is difficult, the treatment is largely agreed upon: surgical resection of the appendix with possible cecectomy.4,16 The greatest concern is the possibility of a malignant cause of intussusception, which can be difficult to rule out with imaging and endoscopic biopsies.13,16 As such, surgical resection is the preferred treatment. However, given that appendiceal intussusception is commonly an incidental finding on colonoscopy, the question of endoscopic resection of the apparent polyp should be addressed. Simple polypectomy poses the risk of bowel perforation at the base of the appendix; however, one study did demonstrate the efficacy of using an Endoloopâ as an alternative to traditional surgical resection.18 Nevertheless, the risk of perforation and the inability to definitely rule out malignant causes make surgery an appropriate treatment plan.
Conclusion
In conclusion, intussusception of the appendix is a rare finding with various presentations. Endometriosis is a rare cause of such pathology, acting as a lead point and sometimes placing the patient at risk for further intussusception. As such, intussusception of the appendix should be included in the differential for vague right lower quadrant pain. Surgical intervention is an appropriate course of action to definitively rule out malignancy and decrease the risk of further intussusception.
Lessons Learned
Appendiceal intussusception is a very rare finding with varied etiologies and presentations, with endometriosis being a particularly rare cause. Appendiceal intussusception should be included in the differential for various abdominal presentations. Surgical intervention is a safe and effective treatment option that can definitively rule out malignancy as the etiology.
Authors
Paolini MJa; Berkey SEb; Liang Jc; Nabi Ed; Bello BLb
Author Affiliations
- Georgetown University School of Medicine, Washington, DC 20007
- Department of Surgery, MedStar Washington Hospital Center, Washington, DC 20010
- Department of Pathology, MedStar Washington Hospital Center, Washington, DC 20010
- Department of Medicine, MedStar Washington Hospital Center, Washington, DC 20010
Corresponding Author
Brian L. Bello, MD, FACS
106 Irving Street NW
Ste. 2100N
Washington, DC 20010
Email: brian.l.bello@medstar.net
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding/Support
The authors have no relevant financial relationships or in-kind support to disclose.
Received: October 21, 2020
Revision received: December 11, 2020
Accepted: February 1, 2021
References
- M'Kidd J. Case of Invagination of the Cœcum and Appendix. Edinb Med J. 1859;4(9):793-796.
- Birkness J, Lam-Himlin D, Byrnes K, Wood L, Voltaggio L. The inverted appendix - a potentially problematic diagnosis: clinicopathologic analysis of 21 cases. Histopathology. 2019;74(6):853-860. doi:10.1111/his.13824
- Collins DC. 71,000 Human appendix specimens. A final report, summarizing forty years' study. Am J Proctol. 1963;14:265-281.
- Ijaz S, Lidder S, Mohamid W, Carter M, Thompson H. Intussusception of the appendix secondary to endometriosis: a case report. J Med Case Rep. 2008;2:12. Published 2008 Jan 22. doi:10.1186/1752-1947-2-12
- Chaar CI, Wexelman B, Zuckerman K, Longo W. Intussusception of the appendix: comprehensive review of the literature. Am J Surg. 2009;198(1):122-128. doi:10.1016/j.amjsurg.2008.08.023
- McSwain B. Intussusception of the appendix review of the literature and report of a case. South. Med. J. 1941;34:263–271.
- Nycum LR, Moss H, Adams JQ, Macri CI. Asymptomatic intussusception of the appendix due to endometriosis. South Med J. 1999;92(5):524-525. doi:10.1097/00007611-199905000-00016
- Howard RJ, Ellis CM, Delaney JP. Intussusception of the appendix simulating carcinoma of the cecum. Arch Surg. 1970;101(4):520-522. doi:10.1001/archsurg.1970.01340280072019
- Schmidt FR, McCarthy JD. Intussusception of the appendix with endometriosis presenting as a cecal tumor. Arch Surg. 1971;103(4):515-517. doi:10.1001/archsurg.1971.01350100113022
- Costa M, Bento A, Batista H, Oliveira F. Endometriosis-induced intussusception of the caecal appendix. BMJ Case Rep. 2014;2014:bcr2013200098. Published 2014 Dec 4. doi:10.1136/bcr-2013-200098
- Birriel TJ, Smith E, Eyvazzadeh D. Appendiceal intussusception from endometriosis: endoscopic and laparoscopic approach. Ann R Coll Surg Engl. 2017;99(1):e1-e2. doi:10.1308/rcsann.2016.0244
- Lee DJ, Kim HC, Yang DM, et al. A case of intussusception of the appendix secondary to endometriosis: US and CT findings. J Clin Ultrasound. 2015;43(7):443-446. doi:10.1002/jcu.22188
- Akagi T, Yamamoto S, Kobayashi Y, et al. A case of endometriosis of the appendix with adhesion to right ovarian cyst presenting as intussusception of a mucocele of the appendix. Surg Laparosc Endosc Percutan Tech. 2008;18(6):622-625. doi:10.1097/SLE.0b013e318180f67f
- Dickson-Lowe RA, Ibrahim S, Munthali L, Hasan F. Intussusception of the vermiform appendix. BMJ Case Rep. 2015;2015:bcr2014207584. Published 2015 Jul 16. doi:10.1136/bcr-2014-207584
- Manoharan B, Haider AS, Samira AM, Bharathan B, Parra-Blanco A. Isolated appendiceal endometriosis resulting in intussusception. Oxf Med Case Reports. 2018;2018(10):omy099. Published 2018 Sep 26. doi:10.1093/omcr/omy099
- Mehmood S, Phair A, Sahely S, et al. Appendiceal intussusception caused by endometriosis. Lancet. 2012;380(9848):1202. doi:10.1016/S0140-6736(12)60819-8
- Jubanyik KJ, Comite F. Extrapelvic endometriosis. Obstet Gynecol Clin North Am. 1997;24(2):411-440. doi:10.1016/s0889-8545(05)70311-9
- Matsushita M, Nishio A, Seki T, Okazaki K. Inverted Appendix: Final Diagnosis or Endometriosis?. Am J Gastroenterol. 2016;111(5):746. doi:10.1038/ajg.2016.69
- Liang HH, Huang MT, Wei PL, et al. Endometriosis-induced appendiceal intussusception. Am J Surg. 2009;197(6):e66-e68. doi:10.1016/j.amjsurg.2008.04.024