The patient subsequently underwent partial mastectomy and sentinel node biopsy with final anatomic and pathologic stage of IIA and IA, respectively (AJCC8). She completed adjuvant radiation therapy and is currently taking adjuvant endocrine therapy for a prescribed time of five years. Workup of the hyperparathyroidism was placed on hold during her treatment. She is experiencing some hot flashes on endocrine therapy but otherwise feels asymptomatic from her hyperparathyroidism and has elected to delay surgery at this time.
Discussion
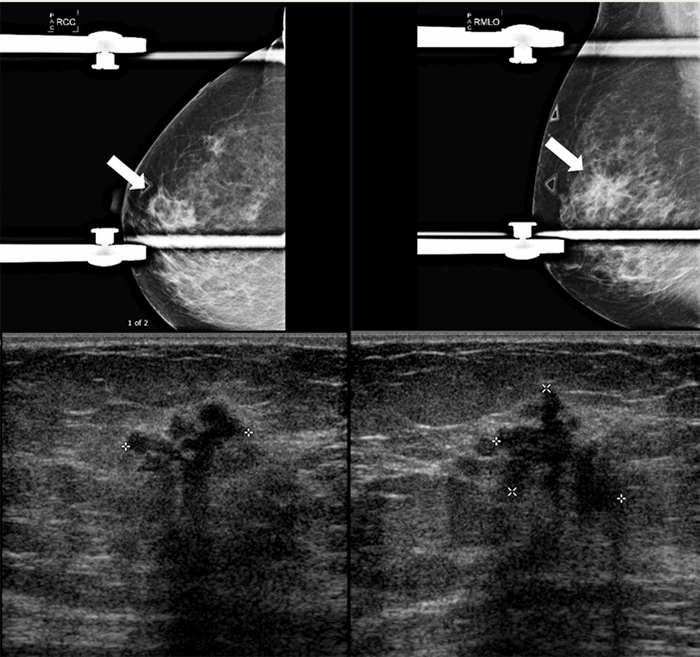
The current screening and diagnostic imaging methods for breast cancer include mammography, ultrasound, and MRI. Mammography and MRI in particular have demonstrated relatively high sensitivity and specificity across the general patient population; however, there have been specific limitations reported with both.
Mammography sensitivity can have wide variations depending on breast density, ranging from 48 percent sensitivity for women with very dense breast compared to 78 percent sensitivity for all women.3 With breast density being one potential factor for imaging occult breast cancers, it is important for imaging methods to not be restricted by this factor. Breast density is now incorporated into risk calculators for breast cancer, and low-cost imaging modalities are constantly under evaluation to aid in detection of breast cancer in dense breasts.
MRI scans can compensate for some of the limitations exhibited with mammography, such as breast density. However, there have been varying sensitivity results reported with MRI. Although sensitivity for cancer detection with breast MRI is high (over 90 percent), specificity is low to moderate (72 percent). The relatively low specificity of MRI can make differentiating between benign and malignant findings challenging, leading to a high number of biopsy recommendations.4 Furthermore, MRI is more expensive than both CT and mammographic imaging.
This case study demonstrates the ability of gamma imaging with technetium-99m-sestamibi to detect breast lesions. Sestamibi scans are traditionally used for localization of parathyroid adenomas in a 3-dimensional field.5 The abnormal parathyroid gland readily uptakes 99mTc-sestamibi due to the increased number of mitochondria in the environment.6,7 This allows surgeons to localize and assess the size of the gland for surgical excision.
However, in the case of this patient, the authors were able to identify an incidental malignant mass in the right breast. A number of studies have explored the diagnostic potential of 99mTc-sestamibi in breast cancer using scintimammography. In a study by Maublant et al., the authors analyze 198 tumors and demonstrate markedly increased 99mTc-sestamibi concentrations in the breast tumor in addition to some affected lymph nodes.8 The amount of uptake in tumors appears to be dependent of tumor size, as quantified in the study by Tan et al.9 A large metanalysis by Xu et al. demonstrated that for patients who exhibited a palpable mass, the sensitivity and specificity of 99mTc-sestamibi scintimammography were 87 percent and 86 percent, respectively. Patients without palpable masses had a sensitivity and specificity of 59 percent and 89 percent, respectively. The overall findings indicated 99mTc-sestamibi scintimammography nuclear imaging as a viable option for breast cancer diagnosis.10 With the evidence thus far, 99mTc-sestamibi scintimammography imaging may be a viable adjunctive imaging modality to be used with mammography, particularly in patients with dense breasts who exhibit lower sensitivity and specificity with standard mammography. There are now commercially available, breast specific 99mTc-sestamibi gamma imaging machines available.
Conclusion
Numerous breast cancer imaging modalities exist; however, there are limitations to each method. The authors present a case that demonstrates the ability of sestamibi scan for hyperparathyroidism to detect incidental breast lesions. It highlights the need to further explore the value and limitations of sestamibi scans in relation to other common imaging technique such as mammography and MRI.
Lessons Learned
The imaging modality 99mTc-MIBI parathyroid scintigraphy can detect breast cancer lesions. Additionally, it may accurately detect breast cancers, especially when used in conjunction with other imaging modalities.
Authors
Grisham CJa; Sanders Mb; Langdon Wc; Baregamian Na; Sweeting RSa
Corresponding Author
Raeshell S. Sweeting, MD
597 Preston Research Building
Vanderbilt University
2220 Pierce Avenue
Nashville, TN 37232
Phone: (615) 322-2391
E-mail: raeshell.s.sweeting@vanderbilt.edu
Author Affiliations
a Division of Surgical Oncology & Endocrine Surgery, Vanderbilt University Medical Center, Nashville, TN 37232
b Department of Pathology, Microbiology & Immunology, Vanderbilt University Medical Center, Nashville, TN 37232
c Department of Radiology, Vanderbilt University Medical Center, Nashville, TN 37232
Meeting Presentation
Tennessee Chapter of the American College of Surgeons, Nashville, TN, August 2018
Disclosure Statement
The authors have no conflicts of interest to disclose.
References
- McPherson K, Steel CM, Dixon JM. ABC of breast diseases. Breast cancer-epidemiology, risk factors, and genetics. BMJ. 2000;321(7261):624-628. doi:10.1136/bmj.321.7261.624
- Etzioni R, Urban N, Ramsey S, et al. The case for early detection. Nat Rev Cancer. 2003;3(4):243-252. doi:10.1038/nrc1041
- Kolb TM, Lichy J, Newhouse JH. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology. 2002;225(1):165-175. doi:10.1148/radiol.2251011667
- Baltzer PA, Benndorf M, Dietzel M, Gajda M, Runnebaum IB, Kaiser WA. False-positive findings at contrast-enhanced breast MRI: a BI-RADS descriptor study. AJR Am J Roentgenol. 2010;194(6):1658-1663. doi:10.2214/AJR.09.3486
- Eslamy HK, Ziessman HA. Parathyroid scintigraphy in patients with primary hyperparathyroidism: 99mTc sestamibi SPECT and SPECT/CT. Radiographics. 2008;28(5):1461-1476. doi:10.1148/rg.285075055
- Sandrock D, Merino MJ, Norton JA, Neumann RD. Ultrastructural histology correlates with results of thallium-201/technetium-99m parathyroid subtraction scintigraphy. J Nucl Med. 1993;34(1):24-29
- Anand SS, Chauhan MS, Singh J. Preoperative Parathyroid Radionuclide Scintigraphy in Hyperparathyroidism. Med J Armed Forces India. 2005;61(1):74-75. doi:10.1016/S0377-1237(05)80126-1
- Maublant J, de Latour M, Mestas D, et al. Technetium-99m-sestamibi uptake in breast tumor and associated lymph nodes. J Nucl Med. 1996;37(6):922-925.
- Tan H, Zhang H, Yang W, et al. Breast-specific gamma imaging with Tc-99m-sestamibi in the diagnosis of breast cancer and its semiquantitative index correlation with tumor biologic markers, subtypes, and clinicopathologic characteristics. Nucl Med Commun. 2016;37(8):792-799. doi:10.1097/MNM.0000000000000518
- Xu HB, Li L, Xu Q. Tc-99m sestamibi scintimammography for the diagnosis of breast cancer: meta-analysis and meta-regression. Nucl Med Commun. 2011;32(11):980-988. doi:10.1097/MNM.0b013e32834b43a9