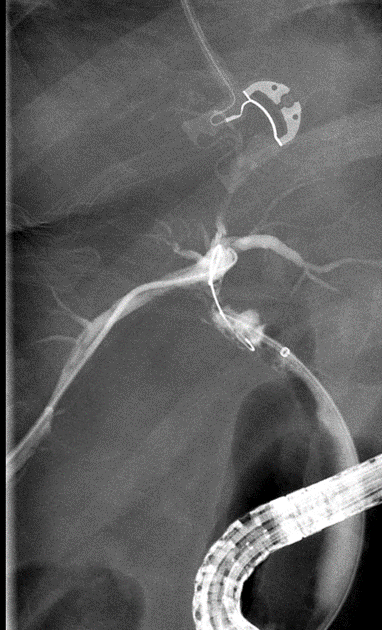
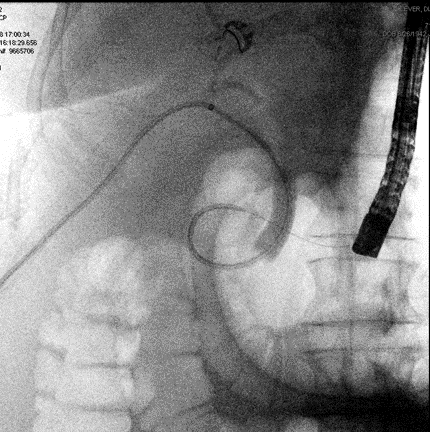
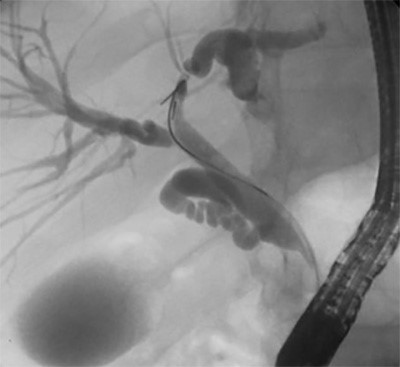
Figure 7. Final rendezvous cholangiogram showing flow through PTBD through the previous biloma cavity, cystic duct and CBD, finally into the duodenum.
The patient went on to do well. PTBD was capped two days following the procedure and her bilirubin levels remained low. Her AKI was reversed, and her electrolytes normalized with good nutrition. She was able to be discharged a week following the procedure with daily PTBD flushes and drain care. Ultimately, the goal will be complete internalization of the drain, so she doesn't have to have a cap on her skin once an epithelialized tract has formed.
Discussion
Traditional surgical approaches to bile duct injuries (BDI) include Roux-en-Y hepaticojejunostomy (RYHJ) and potentially liver resection depending on extent and classification of injury. Type C injuries, as described here, pose a specific challenge as there is often a very short, small caliber external portion of extrahepatic duct and variable blood supply. Therefore, liver resection is often necessary to stop the bile leak. Both RYHJ and liver resection are major surgical procedures that can be life threatening for poor surgical candidates. In addition, as illustrated in this case, these patients are made even more medically fragile by their BDI due to dehydration, malabsorption and electrolyte disturbances. By involving a multi-disciplinary team of HPB surgeons, IR, and GI with ERCP experience, the options for treatment widen with less risk of major complication. Often stenting via ERCP by an endoscopist, or an internalized PTBD with interventional radiology, may be enough to control a bile leak post cholecystectomy. The goal of these attempts being to decompress the biliary tree and allow healing of the defect.
A rendezvous procedure refers to the combination of endoscopic, percutaneous and/or surgical approaches to achieve a goal through 2 points of the body that cannot be achieved via one. This method is often used for patients with hepatobiliary dysfunction, when ERCP or PTBD alone are not sufficient for achieving desired outcomes.1
A few similar cases of combined percutaneous/endoscopic/operative Rendezvous Procedures for CBD injuries have been described.2 Sathyanarayana et al3 described what they believed to be the first 2 cases in the literature in 2014. Their patients both had extensive biliary injuries (type E4) who were unable to have internalized drainage and the IR team came into the OR to participate in the surgeries.
Elmunzer et al4 describe a rendezvous procedure for a complete bile duct transection (E2 injury) in which a fully covered, self-expanding metallic stent (SEMS) was inserted into a previously formed PTC rendezvous tract. When the stent was removed 6 months later, a cholangiogram showed no stricture or leak (she did re-stricture 3 months later requiring another round of 5 months of stent therapy). Interestingly, in our case, no fibrotic tract was present across the biloma cavity, but a wire was still able to be manipulated across it. This was due to recanalization of the cystic duct after about 2.5 months, causing it to communicate with the biloma despite likely being stapled intraoperatively.
In a slightly different example of a Rendezvous Procedure, Meek et al5 outline a maneuver performed solely by IR in which 2 separate percutaneous access routes were used to pass a glidewire across a biloma cavity and create continuous access from the intrahepatic ducts into the CBD. This modification of the Rendezvous would be useful in patients in whom endoscopy options are limited, for example post Roux-en-Y gastric bypass.
Conclusion
This case describes the use of a Rendezvous Procedure to establish biliary-enteric continuity in a patient who was deemed to be an unfit surgical candidate for repair of a type C common bile duct injury post cholecystectomy. Interdisciplinary coordination was necessary to come up with an individualized stepwise treatment plan when PTBD internalization was not possible. Bile duct injury following cholecystectomy is challenging to treat, in part because each patient, and every injury, is distinct and liver anatomy is rarely cookie-cutter. Combined Rendezvous Procedures, planned in cooperation with hepatobiliary surgeons and executed by a multi-disciplinary team, add a potentially safer option for patients with complex biliary injuries to treatment options.
Lessons Learned
Individualized care of patients with challenging bile leaks and ductal injuries post cholecystectomy should be managed at a center with multidisciplinary care (HPB surgery, GI, and IR) and with experience in complex options for treating these patients.
Authors
Johnathan Righetti, MD
Virginia Mason Medical Center
Seattle, WA
Janelle Rekman, MD
Virginia Mason Medical Center
Seattle, WA
Adnan Alseidi, MD, FACS
Virginia Mason Medical Center
Seattle, WA
Correspondence Author
Johnathan Righetti, MD
Virginia Mason Medical Center
925 Seneca St.
Seattle, WA 98101
Phone: 406-253-0401
Email: Johnathan.righetti@virginiamason.org
Disclosure Statement
The authors have no conflicts of interest or financial disclosures to disclose.
References
- De Robertis R, Contro A, Zamboni G, Mansueto G. Totally percutaneous rendezvous techniques for the treatment of bile strictures and leakages. J of Vasc and Interven Rad. 2014; 25(4): 650-4.
- Shin S, Klevan A, Fernandez C, Astudillo J, Martinez C. Rendezvous technique for the treatment of complete common bile duct transection after multiple hepatobiliary surgeries. J of laparoendoscopic and adv Surg techniques. 2014; 24(10): 728-30.
- Sathyanarayana S, Lee C, Lobko I, Febles A, Madariaga J. Modified rendezvous biliary procedure involving the hepatobiliary surgeon, endoscopist, and interventional radiologist: a novel solution for complex bile duct injuries. J Am Coll Surg. 2014; e51-54.
- Elmunzer B, Feussner D, Payne M, Nadig S, Yamada R. Combined endoscopic-percutaneous biliary restoration following severe bile duct injury during cholecystectomy. Am J Gastro. 2018; 113: 329.
- Meek J, Fletcher S, Crumey K, Culp W, Meek M. Percutaneous rendezvous technique for the management of a bile duct injury. Radiology case reports. 2018; 13: 175-178.
- Strasberg SM, Hertl M, Soper J. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995; 180:101-25.