Discussion
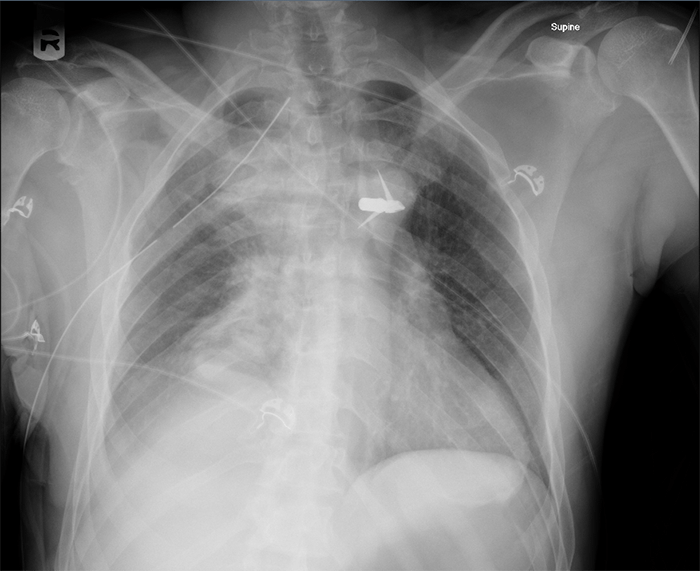
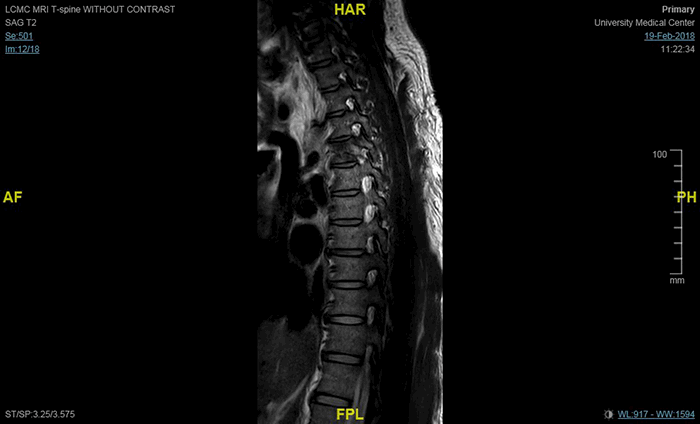
Penetrating trauma from an arrow is an uncommon injury but has a high associated mortality and poses unique challenges in clinical management. When these incidents occur, this mechanism is most commonly the result from accidental firing or suicide attempts, while homicide attempts are least frequently reported in the literature (Table 1).1-13 In our case report, we described the case of a patient who survived a crossbow injury to the chest from a homicide attempt that resulted in a permanent spinal cord injury below T3.
Table 1. Summary of previous studies of crossbow injuries to the midsection
| Author | Anatomic sections involved | Organs injured | Surgical intervention | Injury Intention | Outcome | Post-operative course |
| Besler et al. (1997)1 | L hemithorax, L mediastinum | 1. Left anterior descending artery (LAD)
2. Inter-ventricular septum (IVS) | 1. Median sternotomy without opening pleura
2. Pericardiotomy
3. Removal of bolt from LAD and IVS | Suicide attempt | Full recovery | Uneventful |
| Chang and Hsee (2010)2 | Thorax | 1. L pleura
2. R erector spinae muscle | 1. L chest tube for hemopneumo-thorax
2. Incision of R back to access erector spinae
3. Removal of bolt via advancement anterior to posterior through the muscle | Accidental firing | Full recovery | Uneventful; LOS 3 days |
| Fradet et al. (1988)3 | LUQ, L mediastinum, L hemi-thorax | 1. L lobe of liver
2. Diaphragm
3. Posterior mediastinum
4. Lower thoracic aorta | 1. Thoraco-abdominal incision of L 7th intercostal space
2. Evacuation of 1L of blood and clot in L chest
3. Control of dissected aorta
4. Aortic anastomosis with Gore-Tex
4. Laparotomy for liver injuries | Accidental firing | Full recovery | Uneventful, LOS 8 days |
| Hunt and Sodergren (2017)4 | L thoraco-abdominal cavity | 1. Peri-cardium
2. Diaphragm
3. Liver
4. Distal Pancreas
5. L kidney | 1. Midline laparotomy and pericardotomy
2. Divided arrow below diaphragm
3. Bolt shaft removed from liver
4. Distal pancreatectomy and splenectomy
5. Complete removal of foreign body
6. L renorrhaphy | Suicide attempt | Survival | Discharged POD 7 to psychiatric unit |
| Karger et al. (2004)5 | Thoraco-abdominal cavity | 1. L upper arm
2. Peri-cardium
3. Thorax
4. Stomach
5. Liver | Unknown; surgery survival time 6.5 hrs | Homicide attempt | Death | |
| Kennedy et al. (2012)6 | L hemithorax | 1. Pulmonary hilum
2. Upper lobe of L lung | 1. L anterolateral thoracotomy to control pulmonary hilum bleed
2. Removal of bolt
3. L Chest tube | Unknown | Full recovery | Uneventful; ICU LOS 3 days, then discharged; follow-up 1 month with no complications |
| Koizumi et al. (2014)7 | R anterior thorax, R anterior abdomen | 1. Middle lobe of R lung
2. Diaphragm
3. Liver | 1. R anterior thoracotomy in L lateral decubitus
2. Partial resection of middle lobe
3. Bolt removed from liver through abdominal incision | Suicide attempt | Full recovery | Uneventful; LOS 12 days |
| Kruke-meyer et al. (2005)8 | L thoraco-abdominal cavity | 1. L lung (lobe unspecified)
2. Diaphragm
3. Liver | 1. Massive transfusion
2. Thoracotomy (type not noted)
3. Laparotomy 4. B/l chest tubes
5. Blood transfusion | Homicide attempt | Survival | Complicated stay: POD 13 extubated but continued on intensive respiratory therapy; POD 14 chest tubes removed, stepped down from ICU status; POD 16 discharged to outpatient aftercare |
| Mullan et al. (1991)9 | L hemithorax, L mediastinum | 1. Lower sternum
2. Peri-cardium
3. Anterior wall of right ventricle
4. Inter-ventricular septum
5. Posterior wall of L ventricle
6. Descending aorta | 1. Femoro-femoral cannulation for cardiopulmonary bypass
2. Median sternotomy
3. Aortobicaval cannulation and bypass under profound hypothermia (10-15°C) and intermittent circulatory arrest
4. Exposure of aorta through posterior pericardium
5. Bolt removal
6. Anastomosis of aorta | Suicide attempt | Full recovery | Uneventful; POD 8 patient discharged himself |
| Preiss et al. (2003)10 | L hemithorax | 1. Peri-cardium
2. Myo-cardium
3. Inter-ventricular septum (IVS) | 1. Median sternotomy
2. Pericardotomy, empty pericardium noted
3. Cardiorrhaphy of myocardium and IVS with pericardial patch | Suicide attempt | Full recovery | Uneventful |
| Wan and Kefaloy-annis (2016)11 | L hemithorax | 1. L upper lobe of lung
2. L lower lobe of lung
3. T spine | Posterolateral thoracotomy | Suicide attempt | Unknown | Unknown |
When stratified by location of the injury, transcranial or transorbital were the most frequent locations.8,14-26 These wounds present with unique concerns, including immediate concern for airway compromise,20,21,24,25 necessity for facial reconstruction,22,25 monitoring for significant intracranial hemorrhage14-21 and neurologic injury,14,16-22,24,25 and were usually the result of a suicide attempt.8,13,14,16-19,22,24-26 Patients reported to survive crossbow injuries at a higher rate typically had thoracic or thoracoabdominal impalement. In review of the literature, thoracic wounds remain largely confined to one hemithorax,2,3,6,7,8,11 some involving mediastinal or cardiac injuries,1,3,4,8,9,10 with occasional abdominal involvement.3,4,7 Surprisingly, most patients struck with an arrow below the neck had a relatively normal neurologic exam, presenting with a Glasgow Coma Scale patient score greater than or equal to 13.1,3,5,7,8,9,11,27,28 Thus, spinal cord injury as a result of penetration from an arrow is not well-described. We identified several case reports that describe the arrow’s trajectory in close proximity to the spinal cord. A case report published by Wan et al. describes an arrow traversing a patient’s left hemithorax, damaging both the left upper and lower lobes of the lung, and striking the thoracic spine.11 A case report from Chang and Hsee described a patient with the arrow’s trajectory crossing midline, entering from the left supraclavicular fossa and lodging in the right erector spinae muscle.2 Finally, an additional case report by Kovari in which the shaft traversed the spinal canal, but the cord remained intact. The patient developed mild ataxia, which may have been a result of minor trauma to the spinal cord.29 However, no case reports reported a situation in which the patient’s spinal cord was transected as a result of the injury.
The majority of previously published case reports focused on important features of the mechanism of an injury. Arrows fired from a crossbow, despite their high speed, have less kinetic energy than a bullet.5,6,8,12,13,15,30-34 This important distinction results in difficulty damaging bony structures,5,15,35 thereby reducing the risk of bone fragments.18 A bullet has the kinetic energy to fracture vertebrae and thus injure the spinal cord, whereas the arrow’s pathway must access the cord without being hindered by bony processes. To our knowledge, this case is the first report to detail spinal cord damage from an arrow.
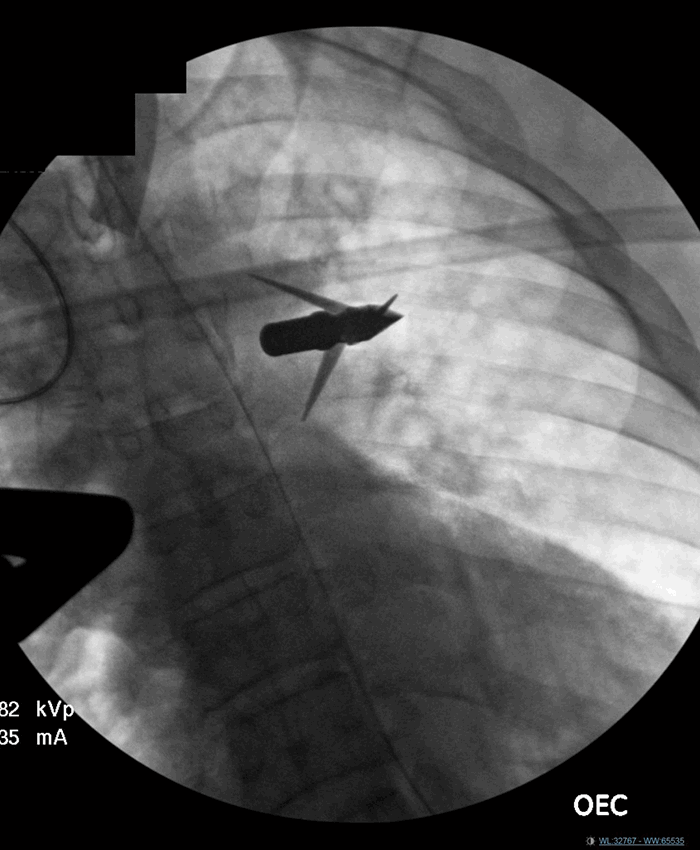
As such, another unique aspect of this case was the operative management involving both trauma and neurosurgical teams was central to minimizing the neurologic deficits in delivering life-saving care. Strategic management of the arrowhead as a tamponade as well as the shaft to facilitate hemostasis is critical. The operative management of the foreign body’s piecewise removal was an essential feature of this case. Some previous case reports described intraoperative detachment of the point from the bolt, leaving only the arrowhead to tamponade the tissue in which it lodged,2,3,6,-9,27,28 in our operation, we applied this concept in a different manner, using the shaft to tamponade. Once proximal hemostasis was achieved, the shaft was divided at its midpoint, facilitating control of hemostasis as well as visualization of deeper injuries: maximizing control over the foreign body’s movement to minimize further damage is essential.2,3,6,-9,27,28 This approach enabled the trauma surgeons to take an anterolateral approach to the thoracotomy, and then the neurosurgeons to remove the arrowhead and address the spinal and muscular wounds from a posterior approach. The neurosurgical team elected to keep the arrowhead attached to the shaft, since arrowhead protruded posterior to the spine. As such, the remaining shaft-and-point remnant was removed from the left posterior thorax. This was similar to the approach reported previously by Chang and Hsee,2 but in our case the bolt had pierced the musculature through-and-through, rather than stopping within the muscle tissue, requiring surgical advancement through a pierced muscle for its removal.
To our knowledge, this patient is the first case of a patient surviving a penetrating crossbow injury involving transection of the spinal cord resulting in permanent neurologic damage. Additionally, factors that distinguish this case from previously published ones include the pathway of the arrow that crossed midline and damaged one lobe of the lung, but no other mediastinal structures, including the great vessels or the heart. Despite the fact that penetrating trauma from arrows are rare, our report highlights several critical aspects of treating these patients. Surgeons should be familiar with the need to have a multi-disciplinary approach to repair the affected organs while minimizing nerve damage, and utilization of a foreign body in hemodynamic control.
Lessons Learned
In the anterior-to-posterior transthoracic penetrating crossbow injury patient, a spinal cord injury must be considered. Foreign body removal requires careful operative planning and a multi-disciplinary approach. As demonstrated in our case, the utilization of the bolt and shaft of the penetrating arrow as a means to temporary tamponade the bleeding in order to achieve hemostasis proximally may minimize blood loss.
Authors
Shana M. Zucker, BA
Tulane University School of Medicine
Department of Surgery
New Orleans, LA
Alison A. Smith, MD, PhD
Tulane University School of Medicine
Department of Surgery
New Orleans, LA
Shahrzad Talebinejad, MD
North Oaks
Department of Surgery
Hammond, LA
Chrissy Guidry, DO
Tulane University School of Medicine
Department of Surgery
New Orleans, LA
Patrick McGrew, MD
Tulane University School of Medicine
Department of Surgery
New Orleans, LA
Clifton McGinness, MD, FACS
Tulane University School of Medicine
Department of Surgery
New Orleans, LA
Juan Duchesne, MD, FACS
Tulane University School of Medicine
Department of Surgery
New Orleans, LA
Rebecca Schroll, MD, FACS
Tulane University School of Medicine
Department of Surgery
New Orleans, LA
Correspondence
Shana Zucker
Tulane University School of Medicine
1430 Tulane Ave, Dept. of Surgery, SL-22
New Orleans, LA 70112
Phone: 847-641-1431
Email: szucker@tulane.edu
Disclosures
The authors have no conflicts of interest to disclose
References
- Besler K, Kleiber M, Zerkowski HR, Trübner K. Non-lethal penetrating cardiac injury from a crossbow bolt. Int J Legal Med. 1998;111(2):88-90.
- Chang WK, Hsee LC. Crossbow injury in a developed country. Injury. 2010;41(10):1090-2.
- Fradet G, Nelems B, Müller NL. Penetrating injury of the torso with impalement of the thoracic aorta: preoperative value of the computed tomographic scan. Ann Thorac Surg. 1988;45(6):680-1.
- Hunt D, Sodergren M. Crossbow bolt injury: an unusual case of penetrating trauma. J R Army Med Corps. 2017;163(5):364.
- Karger B, Bratzke H, Grass H, et al. Crossbow homicides. Int J Legal Med. 2004;118(6):332-6.
- Kennedy RO, Gonzalez RP, Brevard SB. Penetrating thoracic arrow injury: a flashback to the Wild West. Am Surg. 2013;79(11):1226-7.
- Koizumi T, Imamura N, Aruga N, Watanabe H, Nakagawa T, Masuda R, Iwazaki M. Successful Treatment of Penetrating Chest Injury Caused by a Crossbow. Tokai J Exp Clin Med 2014;39(2):64-68.
- Krukemeyer MG, Grellner W, Gehrke G, Koops E, Püschel K. Survived crossbow injuries. Am J Forensic Med Pathol. 2006;27(3):274-6.
- Mullan FJ, O’Kane HOJ, Dasmahapatra HK, Fisher RB, Gibbons JRP. Mediastinal transfixion with a crossbow bolt. Br J Surg. 1991;78(8):972-973.
- Preiss M, Besler K, Zerkowski HR. Suicidal crossbow bolt cardiac injury. Surgery. 2003;133(2):228-9.
- Wan Y, Kefaloyannis E. Penetrating chest injury caused by self-inflicted crossbow arrow traversing the hemithorax. Eur J Cardiothorac Surg. 2016;50(3):580.
- Rogers C, Dowell S, Choi JH, Sathyavagiswaran L. Crossbow Injuries. J Forensic Sci. 1990;35(4):886-890.
- Smyk D. Crossbow injuries: a case report. J Forensic Leg Med. 2009;16(6):343-5.
- Kulwin CG, Denardo A, Khairi S, Payner T. Neurosurgical Management of Self-Inflicted Cranial Crossbow Injury. World Neurosurg. 2018;116:69-71.
- Kondo T, Takahashi M, Kuse A, et al. Autopsy Case of a Penetrating Wound to the Left Cerebral Hemisphere Caused by an Accidental Shooting With a Crossbow. Am J Forensic Med Pathol. 2018;39(2):164-168.
- Ishigami D, Ota T. Traumatic Pseudoaneurysm of the Distal Anterior Cerebral Artery Following Penetrating Brain Injury Caused by a Crossbow Bolt: A Case Report. NMC Case Rep J. 2018;5(1):21-26.
- Panata L, Lancia M, Persichini A, Scalise pantuso S, Bacci M. A crossbow suicide. Forensic Sci Int. 2017;281:e19-e23.
- Zyck S, Toshkezi G, Krishnamurthy S, et al. Treatment of Penetrating Nonmissile Traumatic Brain Injury. Case Series and Review of the Literature. World Neurosurg. 2016;91:297-307.
- Xiao J, Bennett GJ, Lutske ME, Belles WJ, Guo WA. Oral, maxillary, and cranial impalement injury by a crossbow arrow. Surgery. 2016;159(4):1234-5.
- Hengzhu Z, Enxi X, Lei S, Xiaodong W, Lun D. A rare case of penetrating brain injury by crossbow in a 22-month-old child. Pediatr Emerg Care. 2014;30(6):421-3.
- Jain D, Aggarwal G, Lubana P, Moses S. Penetrating craniofacial arrow injury. J Neurosci Rural Pract. 2010;1(1):17-9.
- Osborne SF, Papchenko T, De souza CF, Polkinghorne PJ, Hart R. Orbital crossbow injury. Clin Experiment Ophthalmol. 2009;37(5):527-9.
- Pomara C, D'errico S, Neri M. An unusual case of crossbow homicide. Forensic Sci Med Pathol. 2007;3(2):124-7.
- Kaye K, Kilgore KP, Grorud C. Transoral crossbow injury: an unusual case of central nervous system foreign body. J Trauma. 2004;57(3):653-5.
- Joly LM, Oswald AM, Disdet M, Raggueneau JL. Difficult endotracheal intubation as a result of penetrating cranio-facial injury by an arrow. Anesth Analg. 2002;94(1):231-2, table of contents.
- Byard RW, Koszyca B, James R. Crossbow suicide: mechanisms of injury and neuropathologic findings. Am J Forensic Med Pathol. 1999;20(4):347-53.
- Grellner W, Buhmann D, Giese A, Gehrke G, Koops E, Püschel K. Fatal and non-fatal injuries caused by crossbows. Forensic Sci Int. 2004;142(1):17-23.
- Zátopková L, Hejna P. Fatal suicidal crossbow injury—the ability to act. J Forensic Sci. 2011;56(2):537-40.
- Kovari VZ. Successfully treated transoral crossbow injury to the axial spine causing mild neurologic deficit: case presentation. Eur Spine J. 2017;26(Suppl 1):24-30.
- Cina SJ, Radentz SS, Smialek, JE. Suicide using a compound bow and arrow. Am J Forensic Med Pathol. 1998;19(1):102-105.
- Downs JCU, Nichols CA, Scala-Barnett, D, Lifschultz, BD. Handling and Interpretation of Crossbow Injuries. J Forensic Sci. 1994:39(2):428-445.
- Wilson CI, Altschul S, Mead A, Flannagan LM. Bloodstain pattern analysis in a case of suicide with a compound bow and arrow. Am J Forensic Med Pathol. 2004;25(1):80-2.
- Frank M, Schikorr W, Tesch R, et al. Ballistic parameters and trauma potential of pistol crossbows. Int J Legal Med. 2013;127(4):777-82.
- Gresham, GA. Arrows of Outrageous Fortune. Med Sci Law. 1977;17(4)239-240.
- Sung L, Kesha K, Hudson J, Root K, Hlavaty L. Morphology of Modern Arrowhead Tips on Human Skin Analog. J Forensic Sci. 2018;63(1):140-150.