Become a member and receive career-enhancing benefits
Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
Become a member and receive career-enhancing benefits
Our top priority is providing value to members. Your Member Services team is here to ensure you maximize your ACS member benefits, participate in College activities, and engage with your ACS colleagues. It's all here.
Implications of the KEYNOTE-522 Trial for Patients with Early Stage Triple-Negative Breast Cancer.
Elizabeth A. Mittendorf, MD, PhD, FACS
May 1, 2022
PrintShare
Bookmark
It is important to draw surgeons’ attention to a pending clinical trial that will address whether patients experiencing a pCR require a full year of pembrolizumab.
Immunotherapy is frequently used to treat patients with triple-negative breast cancer (TNBC). Based on the KEYNOTE-355 trial, pembrolizumab, a monoclonal antibody targeting the programmed death-1 (PD-1) receptor, was approved for treating patients with metastatic TNBC that is positive for programmed death-ligand 1 (PD-L1) expression.1 Subsequently, pembrolizumab was approved for use in the preoperative setting for early stage TNBC patients, regardless of PD-L1 status.2,3
The KEYNOTE-522 trial randomized 1,174 patients with clinical T1N1-2 or T2-4N0-2 TNBC to preoperative pembrolizumab plus chemotherapy or placebo plus chemotherapy. Following preoperative therapy, all patients in the trial underwent surgery, then continued pembrolizumab or placebo to complete a year. The trial’s coprimary endpoints were pathologic complete response (pCR) and event-free survival (EFS).
After the first 602 randomized patients underwent surgery, an interim analysis was performed that showed a pCR rate of 64.8% in patients receiving pembrolizumab versus 51.2% in patients receiving placebo, a statistically significant difference.3 The EFS data were not mature. At the fourth planned interim analysis, after 39.1 months median follow-up, the estimated 36-month EFS rate was 84.5% in the pembrolizumab arm versus 76.8% in the placebo arm, a statistically significant difference.2 The trial was, therefore, positive for both primary endpoints, leading the US Food and Drug Administration to approve pembrolizumab in combination with chemotherapy in the preoperative setting for early stage TNBC patients.
The approval of pembrolizumab for use in the preoperative setting is particularly important for surgeons who are often the first provider to see newly diagnosed breast cancer patients. Given the survival benefits, it is critical that surgeons identify patients who are eligible for this preoperative therapy regimen of pembrolizumab plus chemotherapy. As detailed above, the trial enrolled patients with cT1N1-2 or T2-4N0-2 TNBC and the EFS benefits were seen regardless of whether the patient’s tumor expressed PD-L1.2 Therefore, there is no need to send the biopsy specimen for PD-L1 testing to identify patients who may benefit from the addition of pembrolizumab to chemotherapy. The benefit was apparent regardless of the patient’s clinical nodal status, suggesting that all patients who met eligibility criteria potentially benefitted.
When our group at the Dana-Farber Brigham Cancer Center, Boston, MA, initially discussed the trial data, one cohort of interest was patients with cT1c tumors and a negative clinical exam. These patients would have been ineligible to participate in the KEYNOTE-522 trial. In an analysis presented at the Society of Surgical Oncology 2022 International Conference on Cancer Care, we looked at cT1cN0 TNBC breast cancer patients who underwent surgery as their initial intervention to determine rates of pathologic node positivity. In our institutional database, which included 175 cT1cN0 patients undergoing surgery upfront, approximately 15% had pathologically node-positive disease. Similarly, in a cohort of 18,608 patients identified in the American College of Surgeons National Cancer Database, approximately 11% were pathologically node-positive.4
Based on these data, we have begun routinely performing axillary ultrasound to identify patients with nodal disease who may benefit from preoperative therapy with pembrolizumab plus chemotherapy. Another important point for surgeons to recognize is that patients who receive pembrolizumab can experience immune-related toxicities, some of which can be lifelong. In the KEYNOTE-522 trial, immune-related adverse events (irAEs) of any grade occurred in 33.5% of patients receiving pembrolizumab; 12.9% were grade 3 or greater.2 The most common irAEs were hypothyroidism (15.1%) and hyperthyroidism (5.2%). Of importance to surgeons was the 2.6% rate of adrenal insufficiency. The symptoms of adrenal insufficiency can be nonspecific, including nausea, loss of appetite, weight loss, fatigue, hypoglycemia, and hypotension. The diagnosis, therefore, may be difficult to make without additional testing.
The approval of pembrolizumab for use in the preoperative setting is particularly important for surgeons who are often the first provider to see newly diagnosed breast cancer patients.
At the Dana-Farber Brigham Cancer Center, our practice is to check morning cortisol levels at baseline and at completion of the preoperative pembrolizumab before the operation. Patients found to have adrenal insufficiency are referred to endocrinology. The finding of adrenal insufficiency does not instigate a change in the operative plan; however, anesthesia will administer hydrocortisone preoperatively. The Society for Immunotherapy of Cancer has published a comprehensive review of the management of irAEs, but it predated the approval of any immunotherapeutic agent in the neoadjuvant setting, so it does not address this particular question.5 New guidelines to address specifics of preoperative immunotherapy are in development.
KEYNOTE-522 was a critical trial that informed management of early stage TNBC; however, a number of questions remain:
What is the optimal chemotherapy backbone?
What are the biomarkers of response and toxicity?
Do we need to continue a full year of pembrolizumab in patients experiencing a pCR?
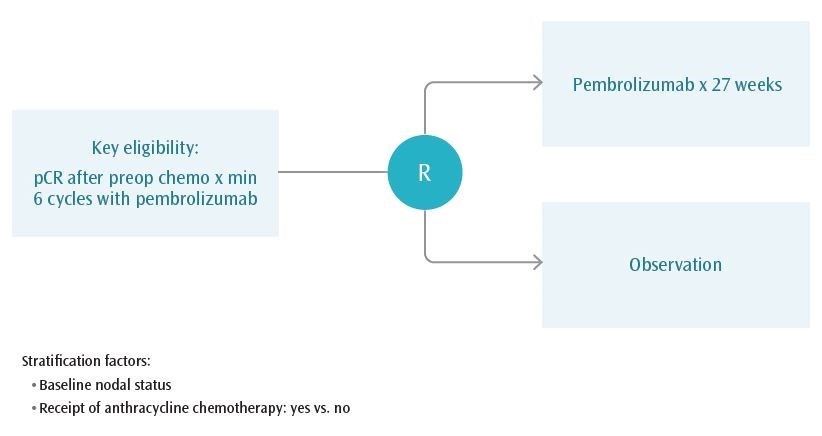
A discussion of these issues is outside the scope of this piece. Nonetheless, it is important to draw surgeons’ attention to a pending clinical trial that will address whether patients experiencing a pCR require a full year of pembrolizumab. This question will be addressed in OptimICE-pCR, a clinical trial led by Sara Tolaney, MD, and the Alliance for Clinical Trials in Oncology. OptimICE-pCR will randomize patients who receive preoperative pembrolizumab plus chemotherapy and experience a pCR to complete a year of pembrolizumab or observation (see Figure 1). The trial’s primary objective is to determine whether observation is noninferior to adjuvant pembrolizumab with respect to invasive disease-free survival. Surgeons are encouraged to consider enrolling their patients with pCR after pembrolizumab plus chemotherapy in this important study.
Figure 1. OptimICE-pCR Trial Schema
References
Cortes J, Cescon DW, Rugo HS, et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): A randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet. 2020;396(10265):1817-1828.
Schmid P, Cortes J, Dent R, et al. Event-free survival with pembrolizumab in early triple-negative breast cancer. N Engl J Med. 2022;386(6):556-567.
Schmid P, Cortes J, Pusztai L, et al. Pembrolizumab for early triple-negative breast cancer. N Engl J Med. 2020;382(9):810-821.
Mittendorf EA, Kantor O, Weiss A, et al. Nodal positivity in early-stage triple negative breast cancer (TNBC): Implications for preoperative immunotherapy. Society of Surgical Oncology 2022 International Conference on Surgical Cancer Care.
Brahmer JR, Abu-Sbeih H, Ascierto PA, et al. Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immune checkpoint inhibitor-related adverse events. J Immunother Cancer. 2021;9(6):e002435.